| Excretion or Inflammation phase | |
| Main remedy: | Gastricumeel |
| Secondary remedy: | Nux vomica-Homaccord |
| Phase remedy: | Hepeel |
Author: Urenus
-
Abdominal bloating
-
Progressive Auto-Sanguis Therapy according to Reckeweg
Introduction and remarks on theoretic aspects
Medical history indicates autohemotherapy’s effects to have first been recognized as a result of the following observation: in persons having sustained blunt traumata with haematoma formation, other affections were also discovered to vanish during the course of haematoma absorbtion. Consequently, therapy with the patient‘s own blood (autohaemotherapy) initially consisted of withdrawing a small quantity of blood from the patient and immediately re-introducing it through intramuscular, hypodermic injection. In this manner, an artificial hematoma was created. The conjecture then was that the injection of one’s own blood would activate defensive powers which, in turn, would combat the ”forces of illness within the blood.” Since then, autohemotherapy has been modified and perfected in multifarious ways, yet in actual practice, the original form of autohaemotherapeutic treatment – as irritation therapy, reversal therapy, non-specific excitation, or stimulation therapy – still finds application in numerous individual cases (e.g., in treatment of acne) with highly successful results.
Progressive auto-sanguis therapy according to Reckeweg is autohaemotherapy in a specialized form. Developed from the fundamentals of homoeopathy in conjunction with Reckeweg’s homotoxicological principles, this technique has proven in practical experience to be reliable and exceptionally effective in treating an extremely wide variety of chronic and degenerative diseases including bronchial asthma, eczema, hepatic damage and numerous other disorders (see also ”Empirically-Proven Indications”).
According to the teachings of Reckeweg’s Homotoxicology, virtually every illness may be defined as either a defensive reaction by the organism against toxins or as the expression of toxic damage. It follows, therefore, that the blood of each patient contains those pathogenic poisons (homotoxins) typical for the disease from which that patient suffers. Through withdrawing a patient’s blood, homoeopathically potentizing it over several levels and subsequently re-introducing it by means of hypodermic injection, Reckeweg holds that precisely these pathogenic poisons undergo modification to yield a homoeopathically active therapeutic agent ideal for application in stimulation therapy. In keeping with the Arndt-Schulz Law in the sense of the inverse effect, this agent stimulates the bodily defense systems, thus increasing detoxification and promoting the healing process.
In accordance with Bürgi’s Principle, the addition of appropriate homoeopathic injection preparations intensifies efficacy of the potentized auto-sanguis blood to an even higher degree. When potentizing the patient’s blood during administration of progressive auto-sanguis therapy, therefore, it has proven expedient to employ the homoeopathic preparation which is therapeutically indicated in each individual patient’s case. In summary, progressive auto-sanguis therapy is treatment designed to exert a counteractive effect against exogenic and endogenic homotoxins (including toxic deterioration products from the body’s own cells), thus promoting the healing of chronic disease in a manner harmonious with the laws of nature.
Also discussed in Homotoxicology are further mechanisms of action which play a role in auto-sanguis therapy, the homoeopathic inverse-effect exerted against both auto- antibodies and antigen-antibody reactions in particular. This effect is due to a complement factor which, as a component of the patient’s own blood, is automatically injected in increasing degrees of attenuation during the course of treatment (the so- called complement-inverse-effect; at the 4th level, potentizing of the blood reaches a degree which approximately corresponds to that of C4!).
This would also explain the positive effects in the area of desensitization/hyposensitization which progressive auto-sanguis therapy is frequently observed to achieve in cases of auto-aggressive disease. One must add, however, that no major scientific studies exist on the subject at this time. Presented here, rather, are the results of hypothetical deliberation based on the positive observations made during the course of daily medical practice.
-
Suis-organ preparations
What are suis-organ preparations?
An important component of anti-homotoxic therapy is the suis-organ preparation. These are preferably employed for chronic courses of diseases in the cellular phases. Subsequently, they offer an excellent possibility for the reactivation of organ functions, particularly of elderly patients. The preparations are employed according to the simile principle, that is, the respective preparation of the organ to be treated is applied. Suis- organ preparations contain organic tissues which have been homoeopathically processed, i.e., attenuated and potentized in accordance with Specification 42 of the official German Homoeopathic Pharmacopoeia 1978 (HAB 1) whose primary materials originate from healthy swine. In accordance with their action, the suis-organ preparations can be characterized as organ-specific medications with stimulative properties. The mechanism through which the suis-organ preparations function is based on the organotropic effects of the substances and/or stimulants contained therein.
Keeping of the donor animals and organ acquisition
The following provides detailed information on the rearing and keeping of swine for the purpose of gaining suis-organ preparations: All swine designated for utilization in gaining organ extracts are descendants from the same breeding line, bred in an operation certified for keeping SPF (”specifically pathogen free”) livestock. This operation is monitored at six- week intervals by the governmental veterinary health service having jurisdiction. At a suitable age, the piglets are transferred and raised in a different agricultural facility. On delivery to this rearing operation, an initial examination is performed by the livestock veterinarian, ensuing passage of which the animals are kept separate from other animals, under veterinary surveillance. Animals requiring medicinal treatment due to any affection are excluded from organ extraction. The animals are given vegetable feed produced on the operation’s own premises. Both operational proprietors have agreed by contract to utilize neither animal meals from mammals, nor waste materials as feed. Upon attaining slaughtering weight and passing release-control by the jurisdictional public veterinarian, the swine are transported to the nearest abattoir, which must possess E.E.C. status. In accordance with regulations for meat hygiene, a live examination of the donor animals is then carried out, as well as meat inspection ensuing slaughter. In all meats attaining the rating ”suitable for human consumption,” samples are drawn for the following additional tests: bacteriological inspection, a test for inhibitory substances, as well as serological analysis for brucellosis, leptospirosis, and yersiniosis in accordance with the Zoonosis Recommendations (July 8, 1991) of the German Federal Ministry of Health.
Removal of the required organs is subsequently performed in an area entirely separate from the remainder of the abattoir, which is utilized exclusively for this purpose. The organs obtained in this manner remain under quarantine until all examination findings have been determined. Only then are the extracted organs released for further processing by the quality control department of the Heel company. The organ preparations are first processed by means of potentization, after which sterilization is then carried out. In this manner, the material preserves the character of the living tissue during potentization; also the preparations thus maintain a direct protein correlation with the affected organ. The measures presented here, all of which are additionally documented by means of official veterinary reports, serve to fulfill one objective: to ensure the highest feasible standard of medicinal safety (zoonosis) for the suis-organ preparations.
The swine as a donor animal
The human organism and that of swine demonstrate numerous similarities in the aspects of chemical and biological constitution, thus a situation of homoeopathic similitude exists. The morphological and other biological similarities between the organisms of man and pig have been the topic of repeated reports during the past several decades. An overview of the factors which man and pig have in common as compiled by Kirkman is provided below (Kirkman, R. L. (1989): ”Of Swine and Man: Organ Physiology in Different Species” In: Hardy, M.A. (ed.): Xenograft 25. Elsevier, Amsterdam and others).
Similar characteristics of man and swine (according to Kirkman, 1989):
- Size
- Dietary habits: omnivorous
- Digestive physiology
- Nephritic structure and function
- Rate and volume of respiration
- Location of the coronary arteries
- Hemodynamics
- Tendency to create fat deposits
- Highly susceptible to disease
- Social behaviour
From the homoeopathic point of view, therefore, despite the difference in species, an organ preparation acquired from swine and subsequently processed in accordance with homoeopathic techniques may be deemed a simile to the homologous human organs due to the numerous existing functional and structural similarities. As Reckeweg observed, it is on the grounds of these similarities that organ remedies obtained from swine possess greater efficacy than such derived from cattle or sheep.
Suis-organ preparations: fields of application
The suis-organ preparations are employed in treatment of the homologous human organs. The Commission D, the committee in the German Federal Ministry of Health concerned with medicinal processing with jurisdiction over homoeopathy, included the following excerpt in their definition of characteristics for organ preparations manufactured in accordance with the German Homoeopathic Pharmacopoeia, HAB 1: ”Homoeopathically- processed organ preparations are applied on the concept that insufficiency or disturbance of the homologous target-organ in humans shall receive succor through the corresponding organ-medication.” Further, the applicational fields are designated by this commission as ”supportive therapy in cases of insufficiency or disturbance of the homologous human organ.”
The suis-organ preparations are indicated particularly, and primarily, in treatment of cellular phases, especially for chronic affections (i.e., the phases of impregnation, degeneration, and dedifferentiation). Yet these remedies may certainly also find application in phases located to the left of the biological division, e.g., in therapy of pathologically disturbed excretion phases (hyperhidrosis, dysmenorrhea, constipation, eliminatory weakness of the kidneys, etc.) One should also bear in mind that therapy with suis-organ preparations is indicated in treatment of numerous deposition phases as well, such as rheumatic diseases, myomas, adiposis, calculi, and the like.
Dosage and modes of administration
The following table presents a general therapeutic plan for the application of suis-organ preparations in treatment of chronic and/or degenerative organic damage.
Fig. 9
Approximate Periods Approx. Periodes 3-4 weeks Preliminary treatment with detoxification agents, i.e. Hepeel, Lymphomyosot, Galium-Heel, Engystol N, Psorinoheel, Ubichinon compositum, Coenzyme compositum etc. 4-5 weeks Suis-organ preparations administered 1-2 x weekly 8i.m.; s.c., i.d., at acupuncture points, orally or as progressive auto-sanguis therapy; initially in injeel form,
after 6-8 injections in injeel-forte form) conjointly with the individually appropriate antihomotoxic remedies.3-4 weeks Suis-organ preparations discontinued. adjuvant anti- homotoxic medication continued alone. Second injection-series with suis-organ preparations as required.
Upon achieving clinical cure, possible reapplication of organ preparations every 2-3 weeks.As indicated in the above table, after four to five weeks’ administration of the suis organ preparations in Injeel form, the Injeel forte form is applied i.m. or s.c. on a trial basis, as a type of test ampoule in order to determine the degree in which the affected organ’s functional regeneration has progressed; i.e., whether the healing process has become largely established at that point in therapy or not. In treating severe degenerative phases as well as in therapeutic attempts for dedifferentiation phases more frequent injections may be required (every 2 – 3 days) in addition to the support of agents which foster and promote regressive vicariation (Galium-Heel, Engystol N, Traumeel S). This is performed most conveniently by means of combination injections. Also frequently expedient are such combination injections utilizing the organotherapeutically-indicated biotherapeutic remedy appropriate in each case (e.g., in conjunction with Hepeel). It often occurs that several suis-organ preparations are indicated in a single patient. This is best performed by syringe, either simultaneously by means of a combination injection, or injected periodically in alternation.
Application of suis-organ preparations through i.v. injection should be initially exercised with restraint. This mode of administration is to be employed only ensuing comparatively lengthy i.m., s.c. or i.d. injection (see above!).
Prior to using the organotherapeutically indicated suis-organ preparation, it is advisable in many cases to apply the corresponding, functionally underlying suis-organ preparation with toxic cleansing (=channeling) action for a period of 2 to 3 weeks, i.e., for the treatment of hepatic disorders, Vesica fellea suis prior to Hepar suis, of the renal disorders Vesica urinaria suis and Ureter suis, as well as Pyelon suis prior to Ren suis etc. In case of severe toxic affliction, the most expedient procedure is to precede usage of the specially indicated suis-organ preparation with application of the organ preparation Colon suis D10, D30, D200 (1-2x weekly i.m. or s.c. for 2 to 3 weeks). Colon suis is beneficial here as it supports and normalizes the eliminatory function of the intestine.
Employment of suis-organ preparations in progressive auto-sanguis therapy
This is appropriate, for example, in treating iatrogenic damage, toxic hepatic damage, migraine, chronic eczema, bronchial asthma, duodenal and ventricular ulcers, arthrosis, as well as lymphatism. See also the related data on hyperimmunization-therapy employing suis-organ preparations (page 44).
Applicational restrictions
Since immunological mechanisms are stimulated through the suis-organ preparations, a stimulative action of the suis-organ preparations is frequently no longer expected in cases of pronounced cachexia and/or marasmus. On the other hand, a possibly occurring focal reaction during the degradation of damaged cells can endanger cachectic and marantic patients in certain circumstances.
Forms in which suis-organ preparations are supplied
For parenteral (and possibly oral; see point 4!) organotherapy, the suis-organ preparations are available in ampoules of 1.1 ml as potency chords in two degrees of strength: as the potency chord D10, D30, and D200, and as the forte form with potency chords D8, D12, D30, and D200. A number of suis-organ preparations are available as single potencies D6 and D200; these are also supplied in ampoules of 1,1 ml. each.
Constituents
In order to conserve space, the entries below have been presented in condensed form. Both degrees of strength – identified in each case through the corresponding addendum ”Injeel” or ”Injeel forte” – contain potency chords and volumes as indicated above.
Example:
Aorta suis-Injeel 1,1 ml injection solution cont.: 0,367 ml each of Aorta suis D10, Aorta suis D30, Aorta suis D200 Aorta suis-Injeel forte 1,1 ml. injection solution cont.: 0,275 ml each of
Aorta suis D8, Aorta suis D12, Aorta suis D30, Aorta suis D200. 1,1 ml. injection solution cont.: 0,275 ml each of Aorta suis D8, Aorta suis D12, Aorta suis D30, Aorta suis D200.Arteria suis-Injeel 1,1 ml injection solution cont.: 0,367 ml each of Arteria suis D10, Arteria suis D30,
Arteria suis D200Arteria suis-Injeel forte 1,1 ml injection solution cont.: 0,275 ml each of
Arteria suis D8, Arteria suis D10, Arteria suis D30, Arteris suis D200.All the suis-organ preparations are formulated in the same general pattern as illustrated here. Prescriptions should always bear the precise designation ”Injeel” or ”Injeel forte” in order to facilitate acquisition of the proper medication through the chemist and wholesaler.
-
Collagen
Collagen is the most abundant protein in man, accounting for 5-6% of adults’ body weight ( Hall, 1964 ). The basic unit of collagen is tropocollagen, a glycoprotein formed by only 4 amino acids (proline, hydroxyproline, glycine, and lysine), organized in a triple helix.
The triple helix (three alpha-chains) of tropocollagen, the basic unit of mature collagen. The molecule is stabilized by the presence in the alpha chains of hydroxylated amino acids whose H+ bonds give it strength and rigidity.
This gives the molecule great strength, rigidity, and flexibility. Tropocollagen gives origin to mature collagen, organized in fibrils and then fibers.
a) Tendon in cross-section [350X magnification (Chèvremont)]. The collagen fibers are grouped in sepimented bundles of different levels.
b) Hierarchical structure of the tendon according to Kastelic et Al., 1978 (reconstructed and updated).
Collagen is a real structure-protein, resistant and flexible.
Collagen fibers play an important role in in the formation of tissues and extracellular matrix, building the scaffold of the body, being the main component of skin, bones, muscles, tendons, ligaments, joint capsules, cartilage, and extracellular matrix.
Optimal joint functionality is ensured by stabilization structures that are found in:
1) the extra-articular compartment (ligaments, joint capsule, tendons, and muscles)
2) the intra-articular compartment (intra-articular ligaments and articular cartilage).Extra-articular restraint apparatus. Four reinforcing overlapped structures (1, 2, 3, 4) cooperate to achieve good articular resistance, providing co-axial articular function or articular function according to the physiological slipping axes.
These structures, which allow stability and locomotion at the same time, consist essentially of collagen.
Therefore, collagen health is necessary for the health of the entire osteo-arthro-myofascial apparatus.
Collagen is also essential for activating the repair processes of all tissues; however, collagen turnover is physiologically very slow.A – Continuity of collagen fibers in the ligament of adult rats. Electron Microscope images from Provenzano P.P. and Vanderby R. Jr. – Collagen fibril morphology and organization: Implication for force transmission in ligament and tendon. Matrix Biology 25(2006) 71-84.
B – Post-traumatic repair of the collagen texture. Electron Microscope images from Provenzano P.P., Hurschler C., Vanderby R. Jr. – Connect. Tiss. Res. 42:123-133, 2001.
Physiologically, the peak of collagen biosynthesis occurs between 45 and 60 years of age. After this age, a quick decrease of collagen is accompanied by a decrease in elastin and proteoglycans as well.
Life curve of the most important macromolecules of the extracellular matrix (H. – Manuale di Medicina Biologica. Regolazione di base e matrice extracellulare. Guna Editore, 2009.” in Heine, 2009)
Aging, trauma, posture problems, and chronic inflammatory diseases damage the integrity and the quality of collagen fibers. Collagen fibers appear no longer organized in a parallel or linear way and may display disruptions and overlapping. This prevents collagen structures from acting properly as mechanical support, or scaffold, of the entire body.
Moreover, a collagen deficiency is always present in inflammatory and/or degenerative diseases of the osteo-arthro-myofascial apparatus and of other structures of mesodermal origin.Collagen in arthro-rheumopathies
Arthro-rheumatic disorders are inflammatory and/or degenerative diseases of the osteo-arthro-myofascial apparatus and of other structures of mesodermal origin such as connective tissue.
It has been estimated that 15-20% of the general population is affected by pathologies of the Musculo-Skeletal System, better defined as arthro-rheumatic disorders, representing 70% of the patients with chronic pain.
In modern societies characterized by an increase of factors such as longer life expectancy, overweight, amateur and professional sport activities, unhealthy diet and incorrect use of drugs, the incidence of these pathologies is rapidly increasing, and will increase in future.All arthro-rheumatic disorders are characterized by collagen deficiency/ disorders (decrease and degeneration of collagen neo-synthesis).
After 50 years of age, collagen synthesis decreases dramatically. The weakening of collagen fibers causes laxity in the anatomical structures needed to contain and stabilize the joints. As a result, joint hypermobility, especially in non-physiological directions and angles, causes joint pain and leads to a progressive degeneration of cartilage and tendons.
Therefore, the primary cause of joint pain is the weakening of collagen structures in the extra articular compartment and in those joints (shoulder, hip, knee) that have intra-articular ligaments. Joint hypermobility, joint overload and misuse increase mechanical stress and cause overuse processes, which are associated to inflammation in the intra-articular and extra-articular compartment.
The treatment of arthro-rheumatic disorders usually consists of a combination of:
1) non-pharmacological treatments (e.g. ultrasound therapy, magnetotherapy, laser therapy, tecar therapy, TENS, acupuncture, moxibustion, massages, etc.).
2) osteopathic and rehabilitative treatments, associated with a change in lifestyle (diet, exercise, etc.).
3) pharmacological treatments, e.g. COXIB, NSAIDs, paracetamol, corticocosteroids, ASA. However, clinical EBM trials highlight that NSAIDs and COX-2 selective inhibitors are useful only for a short time, against symptomatic inflammatory symptoms and are charged of frequent and even strong negative side effects. In the presence of chronic painful diseases, a prolonged use of these drugs inhibits the healing processes causing lack of mechanical strength and serious articular damage in the medium and long term. NSAIDs reduce the synthesis of new collagen. Moreover, the use of these drugs is contraindicated during treatment with oral anticoagulants.
4) Viscosupplementation with hyaluronic acid of different molecular weight into large joints (shoulder, hip, knee), aiming at replacing the hyaluronic acid of the synovial fluid, with lubricating and cushioning effect on the intra-articular compartment.
5) Surgical treatment: prosthesis or fixation (arthrodesis).
6) Guna Collagen Medical Devices: an innovative therapeutic tool.
Collagen in Orthopedics, Traumatology, Sport Medicine, Rehabilitative Medicine
Traumatic injuries, just like overuse and aging, damage the integrity of collagen fibers, which appear no longer organized in a parallel or linear way and may display lacerations.
This can be the case of acute muscular, ligament or tendon injuries, so frequent in professional and amateur athletes.
Moreover, continuous micortrauma caused by repetitive stress typical of sports activities also have a detrimental effect of collagen structures.
The damaged tissue undergoes a long recovery process: a short inflammation phase is followed by a proliferative (repair) phase and then a remodeling phase.
During the proliferative phase, the fibroblasts are urged to build and reorganize the scaffold of the extracellular matrix, which is mainly composed of collagen.During the following remodeling phase, it is important to improve the endurance of the damaged tissue, in order avoid future recurrences.
Collagen in Aesthetic medicine
As we age, there is a natural decline in collagen production. There is also an increase in the enzyme collagenase which breaks collagen down.
This results in an overall decrease in the amount of collagen in the dermis. Another factor contributing to decreased collagen levels is free radicals from UV exposure. Areas with less support begin to cave in and wrinkles begin to form. The destruction of collagen is a major contribution to the loss of skin suppleness and structure that occurs with advancing age. -
Catalysts
The use of catalysts of the intermediary metabolism is a specialty of the anti-homotoxic therapy. The substances designated as intermediary catalysts are physiological constituents of cellular respiration and energy production (citric acid cycle, redox systems). In part these are also substances which are formed during other enzymatic conver-sions and/or are catalytically effective in these processes. Damage to enzyme systems is frequently of iatrogenic nature because many conventional pharmaceutical medications are based on the inhibition of enzymes as the active principle. Enzymes especially are impeded in their activity by increasing environmental stress (e.g., by heavy metals or pesticides). Due to the deficiency of enzyme function a backup of metabolites present before the respective enzymatic reaction occurs as well as a lack of substrates to be metabolized after this reaction.
The administration of the corresponding catalysts in homoeopathic preparations is based upon the concept that the metabolic process is activated and that blocked cell or enzyme functions are reactivated. Since enzyme damage expresses itself as chronic and/or degenerative diseases, the application of catalysts is therefore primarily indicated for such diseases.
Catalysts are substances which accelerate the equilibration of chemical reactions without disturbing the balance of the process themselves. The extent to which a catalyst is able to accelerate a reaction is impressive. An increase of the reaction speed by six decimal powers is not uncommon, since one single enzyme molecule is often capable of converting more than 10,000 substrate molecules per second. At the end of a reaction the catalyst remains unchanged and is again available to immediately catalyse the same reaction on the next molecule. The described process is designated as catalysis. When the reactions occur in bio-systems, they are referred to as ”bio-catalysts.“
The catalysis may be additionally increased by activators, but it also may be reduced or blocked by ”poisons“ (homotoxins). The citric acid cycle is the ”turntable of metabolism,“ which represents the principal path of the catabolic metabolism of the pyruvate and/or the acetyl co-enzyme A. It is a basic, closed, reaction path present in humans, animals, and plants; the cleavage products of the carbohydrate metabolism, the oxidative carbohydrate metabolism, the oxidative decomposition of fatty acids and – after transamination – the cleavage products from the protein metabolism as well all end in it. Furthermore, it supplies important elements for synthesis of the organism. In conjunction with the respiratory chain the citric acid cycle is simultaneously the most significant source of energy for the metabolic process. It supplies the hydrogen for the biological oxidation and is thus closely linked to the energy metabolism of the cells.
The elements of the citric acid cycle are Acidum citricum (citric acid), Acidum cis- aconiticum (cis-aconitic acid), Axidum oxalsuccinicum (oxalosuccinic acid), Acidum a- ketoglutaricum (a-ketoglutaric acid), Acidum succinicum (succinic acid), Acidum fumaricum (fumaric acid), Acidum DL-malicum (malic acid) and the salt Natrium oxalaceticum (oxalo-acetic sodium).
The transformation of one carboxylic acid into the next within the citric acid cycle is mediated by enzymes. The involved enzymes may be inhibited conditionally by noxae (e. g., competitive inhibition, final product inhibition, substrate inhibition), which can lead to concentration variations of single acids of the citric acid cycle. This can in turn trigger reactions or blockades with consecutive symptoms or disease manifestations in various tissues.
It must be taken into consideration that catalysts can only act when the milieu is correct. In control systems and metabolic chains not only the hydrogen ion concentration (pH-value) is involved, but the corresponding substrates and ”co-factors“ must also be available. The co-factors include vitamins and trace elements, including certain metal ions. Some catalysts have to be activated first by these co-factors to render them functionable. Metal enzyme complexes are frequently referred to as metallo-enzymes. Some of these metal ions are ”two-faced“ and while enabling the catalysis in small doses, in larger doses they may inhibit or block functions.
For therapeutic application, the term ”catalyst“ is more broadly defined than in physiological contexts; it includes catalysts in a strict sense (enzymes) as well as the respective substrates, intermediary products, and co-factors.
The available preparations may be classified into three groups:
Group A: Acids of the citric-acid cycle and their salts.
Group B: Quinones and their derivatives as well as other intermediary respiratory catalysts.
Group C: Compounds which effect stimulation: biogenic amines, hormones, elements (cerium), botanical extracts (anthocyanins).
General Recommendations
The implementation of bio-catalysts has a strong stimulative effect on patients (e. g., severe tiredness after administration of the remedy). It is recommended to drink at least 2 to 3 liters during the first three days of treatment and to extense refrain from physical activities as well. In addition a low toxin diet is desirable. Signs of a regressive vicariation should not be suppressed but rather excreted through the assistance of biological therapeutic remedies.
Exact timing is of the greatest importance for the implementation of catalysts. False timing may trigger progressive vicariations in some cases. This phenomenon occurs when the body is in an extremely unstable condition or is too weak to be subjected to a stimulation therapy. It must be particularly ensured with patients in a weakened condition that the treatment is very slowly commenced and is not applied with massive doses of remedies.
Example: Begin with 1/2 ampoule orally 2x weekly or 2x weekly dissolve 1 ampoule in 1 1/2 liters of water and drink this solution in small sips throughout the day. The bio- catalysts frequently achieve the desired effect without the occurrence of severe healing crises.
For all catalyst preparations of Group B, a repetition of injections should only be conducted after subsidence of the possible occurrence of initial aggravation and always when complaints recur. Furthermore, a proper drainage is important, that is, for patients with severe toxic affliction, the endogenic defence system should be mobilized before the therapy with catalysts.
Three phases of the bio-regulation therapy can generally be distinguished:
- Stabilization of the disease process, that is, treatment of possible inflammatory processes, whereby, in certain cases, the conventional therapy may not be dis- continued immediately. A stabilization can be achieved through a diet, sensible life style, sufficient exercise, support of the endogenic defence system, etc.
- Supplementation of deficient substances, including vitamins and trace elements, as well as the treatment of present dysbiosis. A weakened organism with severe deficiencies and dysbiosis must be treated first with parenteral vitamin pre- parations. With regard to mineral and trace elements, particularly zinc, calcium, potassium, and magnesium are important.
- Surgical treatment; removal of inflammation centres: e.g., tooth extraction, sanitation of the paranal sinus, removal of amalgam, etc.
Group A catalysts
Acids of the citric acid cycle and/or their salts
General Information
Control systems and metabolic chains can only fulfil their function when all links of the chain are intact; this means for physiological processes that the initial substrate, enzymes, and intermediary products must be adjusted to each other for the individual metabolic process steps (e.g., citric acid cycle). Functional disorders can be generated in the material or dynamic area; the consequences are always reciprocal. The following constellations result there from:
- The initial substrate is quantitatively insufficient or qualitatively altered. Based on the Michaelis Menten relation of the dependency of the catalytic reaction on the available substrate, a dysregulation is given at the initial step.
- An insufficient quantity of the enzyme is available or it is completely lacking. The metabolic process is impeded or obstructed at this point. The product to be catalysed is either insufficiently or not formed at all – the metabolic process chain is weakened or interrupted.
These basic processes occur at many points in metabolic process chains. The cited performance of the chain is always determined by the weakest link – substrate, enzyme, or intermediary product. Due to the situation that, after every enzymatic dysfunction, the subsequent product to be catalysed is no longer sufficiently formed, the intermediary products play an essential role in the further course of the chain reaction. Therefore, during therapy, enzymatic defects should not only be affected with the lacking or deficient enzyme – when at all possible – but should also be specifically treated with the intermediary products behind the enzyme obstruction.
Several enzyme reactions require magnesium or manganese ions as additional activators. Thus, all kinase reactions require magnesium ions for the phosphate transfer, whereas alkaline phosphatases are activated by magnesium and manganese ions and peptidases by manganese. In many cases the magnesium ions can be replaced by manganese ions when necessary. Thus, it makes sense and is understandable that specific therapy with the intermediary catalysts of the citric acid cycle is initiated or combined with an injection of magnesium and manganese ions as phosphate compounds due to the significance of the anorganic phosphate.
Fields of application
All diseases classified as cellular phases (degeneration phases, dedifferentiation phases) and which are consequently characterized by defective enzymatic control, blockages and/or defective cellular oxidation, e.g.:
- Paresis, neuralgia, toxic neuritis, vegetative dystonia, migraine
- Dermatosis, neurodermitis, pruritus (including pruritus vulvae), psoriasis, vitiligo, pemphigus, sclerodermia
- Bronchial asthma
- Gastric and duodenal ulcer, hepatosis, cirrhosis of the liver and injurious hepatic disorders, pancreopathy
- Nephropathy, e.g., nephrosis and chronic nephritis
- Myocardial impairment, angina pectoris, treatment subsequent to myocardial infarction, arteriosclerosis, cerebral sclerosis
- Dysfunction and dysregulation of endocrine glands, e.g., diabetes mellitus, dysthyroidism
- Precancerous and dedifferentiation phases (previously: neoplasm phases) within any tissue whatsoever
- During and ensuing X-ray and radioactive exposure (several enzymes, e.g. the maleate dehydrogenase, are sensitive to radiation)
- Thrombocytopenia, leucopenia
Dosage
Most expedient is the injection of the individual acids of the citric acid cycle and/or their salts in the sequence in which they are generated within the cell during the course of metabolism to reach all possibly existing defects, obstructions, and instances of faulty regulation. It is advisable in such therapy to inject two to three acids (and/or their salts) simultaneously in the form of a combination injection. For reasons of practicality, these injections are best applied either s.c. or i.m.
As magnesium and manganese ions activate a number of enzymatic processes – the kinase reactions in particular, during which phosphate transfer occurs (see subsection
General Information) – the Magnesium-Manganum-phosphoricum-Injeel included in the combination pack is to be administered with the initial (combined) injection.
The injections are generally applied 1-2x weekly. Upon completion of a series – i.e., after 4 combination injections (see below) – catalyst therapy may possibly require interpolation by a treatment-free interval of 2 to 4 weeks until the injections’ effects have subsided. During this period, however, the indicated anti-homotoxic preparations (Injeels, Homaccords, and other Heel combination preparations, as well as suis-organ preparations and nosodes) are to be applied. Indeed these may also be employed in conjunction with the acids/salts of the citric acid cycle even during the injection period.
During the intake of a homoeopathic remedy present symptoms may be temporarily aggravated (initial aggravation). The patient is advised to consult his/her therapist.
Plan of subcutaneous injections
After an application-free interval of 2 to 4 weeks, repetition of this series of injections. Each acid and/or its salt may be injected separately and repetitively in the Injeel-forte form as well. This is indicated primarily when a particularly effective action during one of the combined injections listed above (1 to 4) was achieved. The ampoules contained in this combination should subsequently be applied individually.
The diet should include ample fresh fruit, grape juice, bilberries, and beet root. The latter are rich in anthocyanins (activators of cellular respiration, hydrogen acceptors); also refer to intermediary catalysts, Group C: Myrtillus, Beta vulgaris rubra!
Package sizes
Packages containing 5, 10, 50 and 100 ampoules of 1,1 ml each.
Citric-Acid-Cycle combination pack (contains 9 ampoules of single constituent Injeels + 1 ampoule Magnesium Manganum-phosphoricum-Injeel).
List of group A catalysts
The Injeel preparations contain the following potency chord in all preparations: D10, D30, D200 0,367 ml each. Exception: Magnesium-Manganum-phosphoricum-Injeel D12, D30, D200.
The Injeel forte preparations contain the following potency chord in all preparations D6, D12, D30, D200 0,275 ml each.
Acidum cis-aconiticum-Injeel forte
Acidum succinicum-Injeel forte
Acidum succinicum D4
Acidum citricum-Injeel
Baryum oxalsuccinicum-Injeel forte
Magnesium-Manganum-phosphoricum-Injeel
Acidum fumaricum D6
Magnesium-Manganum-phosphoricum-Injeel forte
Acidum a-ketoglutaricum-Injeel
Natrium oxalaceticum-Injeel
Acidum a-ketoglutaricum-Injeel forte
Natrium oxalaceticum-Injeel forte
Acidum DL-malicum-Injeel forte
Natrium pyruvicum-Injeel forte
Group B catalysts
Quinones as well as other intermediary respiratory catalysts
General information
Organic compounds which contain one or several carbonyl groups (> C=O) play an important role in electron transfer processes such as cellular respiration and redox reactions without direct O2-involvement. These compounds include quinones, hydroquinones, aldehydes, ketones, and carboxylic acids.
Electron transfers which involve oxygen contain radical intermediates. Radicals can counteract condensation processes as they occur in the impregnation, degeneration, and dedifferentiation (neoplasm) phases in particular. Free radicals are short-lived, highly reactive products of metabolism which contain one or more unpaired electrons (molecules, atoms, and ions). In the 1930s William Koch introduced free radicals and the catalytic effects into medicinal research and employed them successfully for the healing of diverse diseases. At that time, the knowledge of the existence of free radicals was developed based on his research.
The quinones possess the special ability to neutralize oxygen radicals. A quinone therapy improves the cellular respiration (biological oxidation).
Toxins which must be removed during the course of a lifetime can be decomposed by oxidation as well. Oxidation signifies the consumption of oxygen and subsequently, the existence of risk of an inefficient metabolism. It is possible to treat the consequences of a faulty regulation with quinones. Quinone therapy sets high standards on the toxic defence system of the organism. The support of the toxin defence system and a deliberate excretion therapy are important. Bonded amino groups can be transferred to carbonyl groups by transamination and are thus mobilized.
The quinones and methylene blue have certain characteristics in common. For example, both possess the capability of representing the enzyme succino-dehydrogenase (dehydrogenation of succinic acid into fumaric acid) under anaerobic conditions. Without oxygen, methylene blue can serve in place of this enzyme as an electron acceptor.
Fields of application
The preparations within Group B are to be applied preferably for clinical syndromes and/or cellular phases to the right of the Biological Division, i.e., for impregnation, degeneration, and dedifferentiation phases (previously: neoplasm phases).
Dosage
Dosage must always be determined on an individual basis, depending on each patient’s findings, state of health, and individual response to these preparations, which can vary considerably from case to case – even in instances of identical diagnosis! It is generally advisable to apply the catalyst preparations of Group B once, perhaps twice, weekly (i.m., s.c., i.c.; when required also in the corresponding acupuncture points and possibly i.v.).
We wish to point out that, as with the nosodes, catalyst preparations from Group B may also be advantageously employed in the therapy of cellular phases by administering them in conjunction with those preparations required otherwise.
Special therapeutic stipulations
- As a rule, Glyoxal and Methylglyoxal should be applied relatively seldom. For this reason, these two preparations should always be allotted an extensive period of time in which to expend their after-effects.
- In cases requiring the use of para-benzoquinone, it is advisable to precede such treatment with approximately 3 applications of hydroquinone
- Quinhydrone should be coupled with a homoeopathic metal preparation, e.g., with Aurum-Injeel, Argentum-Injeel, or Ferrum metallicum-Injeel.
Package sizes
Packages containing 5, 10, 50 and 100 ampoules 1.1 ml each.
List of group B catalysts
The Injeel preparations contain the following potency chord in all preparations: D12, D30, D200 0.367 ml each.
The Injeel-forte preparations contain the following potency chord in all preparations D8, D12, D30, D200 0,275 ml each.
Anthrachinon-Injeel
Naphthochinon-Injeel
Anthrachinon-Injeel forte
Naphthochinon-Injeel forte
Chinhydron-Injeel
Para-Benzochinon-Injeel
Chinhydron-Injeel forte
Para-Benzochinon-Injeel forte
Glyoxal-Injeel
Trichinoyl-Injeel
Hydrochinon-Injeel
Trichinoyl-Injeel forte
Hydrochinon-Injeel forte
Ubichinon-Injeel
Methylenblau-Injeel
Ubichinon-Injeel forte
Methylenblau-Injeel forte
Ubichinon D6; D30
Methylglyoxal-Injeel
Group C catalysts
Other compounds with stimulative action
General Information
Other compounds with stimulative action and catalytic effects on metabolic and respiratory functions include:
Homoeopathically prepared vitamins of the vitamin B-group as well as of vitamin A and vitamin C (in lowest potency D6, respectively) – as co-factors and/or co-enzymes; compounds with other stimulative and catalytic effects, e.g., biogenic amines such as adrenaline, serotonine (5-hydroxi-tryptamine) and histamine (4-(2’-aminoethyl)-imidazol) and/or their precursors such as the amino acids tryptophane (b-indolalanine = precursor of serotonine) and histidine (b-imidazolalanine and/or b-imidazolylalanine = precursor of histamine) as well as the amino acids cysteine (contains sulphur), Acidum L(+) asparagicum and Acidum glutaminicum, further the degradation products of tryptophane indole and scatole (b-methylindole) and the amino acid derivatives guanidine (Imino-urea) and methylguanidine as well as anthozyanins (activators of cell respiration; hydrogen acceptors) and elements (trace element factors), e.g., cesium and cerium (redox catalytic action).
Dosage
Generally, injections are administered 1-2x weekly. The injection of one or several catalysts is only repeated after the effect of the previous injection has subsided. As the healing consolidates injections are generally more seldom required.
Package sizes
Packages containing 5, 10, 50 and 100 ampoules 1,1 ml each. List of group C catalysts
Nosode preparations
Definition of nosode preparations
Nosodes are disease triggering agents whose virulence or toxicity was eliminated through homoeopathic processing, but whose information fully attains the recognition mechanisms and enables corresponding stimulation which promotes healing. We differentiate between auto-nosode preparations and hetero-nosode preparations.
Auto-nosode preparations
These are substances gained from the patient’s own organism such as blood, urine, lachrymal fluid, sputum, pus, stools, or diseased tissue. The initial substances are homoeopathically adjusted and applied to the same patient.
Hetero-nosode preparations
These are substances which do not originate from the own organism. There are:
Viral nosode preparations e.g. e.g.
Herpes zoster-Nosode
Coxsackie A9 and/or Coxsackie B4Bacterial nosode preparations e.g. Tuberculinum
Staphylococcinum StreptococcinumVaccine-nosode preparations
(from microorganisms or vaccines)e.g. Influenza nosode Rabies vaccine Rubeola vaccine Tissue nosodes (from pathologically altered organs and/or tissues and products of metabolism including body secretions) e.g.
Gastritis-Nosode Tonsillitis-Nosode Sinusitis-Nosode
Mastopathia cystica-NosodeSource material
Nosodes are preparations produced according to a homoeopathic processing technique from pathologically altered organs or organic constituents of human or animal origin, further, from non-living cultures of micro-organisms, decomposition products of animal origin, or from bodily fluids containing pathogens or pathological products, e.g., liquor, or puncture liquid. The identity of the source material is verified by a protocol of the specialist’s findings of the operation material or laboratory results and, when required, by certificates of the suppliers of the bacteria and viruses. The HAB (German Homoeopathic Pharmacopoeia) stipulates that the base material for nosode preparations is first sterilized and that it afterwards complies with the sterility control pursuant to the German Pharmacopoeia (DAB 10). The homoeopathic processing is only conducted upon completion of these prerequisites. Nosode preparations are, therefore, neither vaccines, nor sera, nor other such agents; they are remedies exclusively and purely of a homoeopathic nature. Mother tinctures are manufactured from this source material according to regulations 43 or 44.
The definition of the nosode preparations conforms to the definition of material stipulated in § 3 of the German Drug Law, particularly in items 3 and 4. Thus substances within the meaning of the law are:
- Chemical elements
- Plants and botanical components
- Bodies of animals, including those of living animals as well as body parts, com- ponents thereof and metabolic products of human or animal origin in a proces- sed state
- Microorganisms including viruses as well as their components or metabolic products
There are two different directives for the production of nosode preparations, namely the HAB 1 (German Homoeopathic Pharmacopoeia) specification 43 for mother tinctures from pathologically altered organs or organic components of human or animal origin and specification 44 for mother tinctures from non-living cultures of microorganisms or from decomposition products of animal organs or from bodily fluids containing pathogens or pathological products.
The following examples illustrate the production of nosode preparations:
Viral nosode preparations
Coxsackie-Virus-B4-Nosode This is produced from dead Coxsackie-B4 viruses adjusted to 109 plaque-forming units per milliliter. Herpes Zoster-Nosode This is produced from dead Herpes-Zoster viruses adjusted to 106 plaque-forming units per milliliter Bacterial nosode preparations
Bacterium coli-Nosode This is a preparation produced from Escherichia-coli bacteria cultures adjusted to a specific titer (107 KBE/g). Bacterium lactis aerogenes-Nosode This is a nosode preparation produced
from an Enterobacter-aerogenes bacteria culture (107 KBE/g).Tissue nosodes
Tonsillitis-Nosode This is produced from surgically removed inflamed tonsils (Tonsilla palatina). Gastritis-Nosode This is produced from gastric mucous removed surgically from a gastritis patient Sinusitis-Nosode This is a mucous mass gained from inflamed sinuses. Otitis media-Nosode The source material is pus from patients suffering from a middle ear infection General application information
Nosode preparations are applied according to the
- symptomatic/anamnestic similarity (simile principle) and
- applied at the end and/or after a previously overcome acute illness.
The following remarks refer to the above items:
To a.
The application of the nosode preparations should be administered according to the symptomatic similarity, that on the basis of the fundamental homoeopathic rules of similitude and/or according to the anamnestic etiological similarity to a past illness which has apparently since been cured. The preparation Diphtheria-Nosode (Diphtherinum-Injeel and forte), for example, is not employed primo loco in treatment of acute diphtheria – which would correspond to a similarity to a developing acute infection – but rather for the treatment of cardiac diseases displaying similar symptoms as are present in a heart damaged by diphtheria (= symptomatic similarity) and/or for the treatment of heart-disease patients whose case history includes diphtheria (= anamnestic etiological similarity).
The following is important when employing nosode preparations under the aspect of current etiological similarities:
All nosodes may be used specifically, i.e., as isotherapeutic agents of the corresponding affections from which they were developed. Generally, they are administered in this case as an intermediary remedy in addition to the indicated homoeopathic remedies, whereby particularly excretive, matrix-channeling anti-homotoxic remedies, (e.g. Lymphomyosot, Galium-Heel), play an important role.
To b.
After the disease has been overcome, nosodes are excellent to induce the toxins deposited in the matrix to be excreted more rapidly. Quite frequently, the toxins removed through this technique are not the sole causative agents but also remnant deposits of contagion with latent pathogenic foci as well as colonies of agents which are no longer pathogenic (sources of continuous exudation). This applies particularly with regards to the infectious diseases such as measles, rubella, varicella, influenza, erysipelas, scarlet fever, typhoid fever, diphtheria etc. It can also be assumed that the specific defence processes against the pathogens are reinduced by the nosode preparations. The clinical confirmation of this immuno-modulative effect is found in the regression of currently forced antibody formations as the expression of the incomplete toxin release of the pathogens. Thus the normalization of a pathologically increased antistreptolysin titer is frequently observed after the application of the streptococcus nosode.
Indications for a nosode therapy
- Chronically exudative diseases
- Chronically proliferative diseases
- Degenerative diseases
- Auto-aggression diseases (Caution!)
- Iatrogenic damages
Nosodes may be designated as terrain remedies. Therefore, they are particularly indicated for the treatment of dyscrasia, i.e., constitutional diseases and/or summation states of integrating and/or integrated dispositions. In terms of Homotoxicology, they are useful for cellular phases, especially for re-toxically inhibited phases, for the treatment of auto- aggression diseases (Caution!), of psoric diseases according to Hahnemann, as well as allergies. Auto-aggression diseases should only be treated after corresponding pre- treatment, such as excretion therapies with matrix-channeling anti-homotoxic remedies. Nosodes are not only indicated however for cellular phases but also frequently for humoral phases, particularly when a dyscrasic component is involved or complications threaten to arise or in case of reduced immunopotency.
The effect of nosodes results in terms of a positive vicariation in detoxification and excretion of homotoxins. This signifies simultaneously an increase of the self-healing processes controlled by the defence system. In most cases a summation of known and possibly unknown poisonous substances (homotoxins) is to be assumed, and based on this knowledge is also the necessity and justification of a simultaneous application of a series of nosodes (e.g., Diphtherinum + Psorinum + Medorrhinum), which are to be applied possibly in conjunction with other single-constituent Injeels, combination preparations etc. as a broad spectrum anti-homotoxic remedy in order to cleanse the cited terrain.
Psorinoheel N (drops, ampoules) is, for example, such a broad spectrum nosode preparation which also contains, aside from the two Psora-nosode preparations (Psorinum and Medorrhinum), vaccininum and bacillinum, furthermore two constitution remedies (sulphur and thuja) and a series of additional homoeopathic remedies. This combination preparation is primarily indicated for the phases of the constitution, i.e., for the cellular phases, as well as for the disposition phases or humoral phases. In case of unclear clinical syndromes and/or clinical syndromes which cannot be immediately clarified, with regard to the anamnestic etiological similarity as well as with regard to the symptomatic similarity, it is frequently advisable to include such a combination preparation based on nosodes in the therapy plan particularly for the cellular phases.
Nosodes exercise a profound constitutional effect. Virtually every type of therapy can be effectively reinforced with nosode preparations. They frequently fulfil the role of a missing link in a chain of therapeutic reactions, whereby cure without nosodes is inconclusive or can only be achieved with extreme difficulty. The effect occurs thereby via subliminal antigen-antibody-reactions as well as via the homoeopathic counteracting mechanism of co-repressors.
Dosage
As a matter of principle, dosage is always to be determined strictly on an individual basis, depending upon each patient’s findings, state of health and particular response to each of the nosode preparations, all of which can vary considerably from case to case. In general, dosage consists of 1 ampoule, administered 1 to a maximum of 3x weekly. The duration of therapy with nosode preparations is also to be determined individually, and is to be adjusted in keeping with each given case. A brief interval of treatment (approximately 2 – 4 weeks) is recommended when applied in the aftermath of an acute affection, whereas chronic disorders should receive therapy over a relatively extensive period (approximately 6 months) depending upon the individual reactive condition of each patient.
It is recommended to begin nosode therapy with the normal Injeel form, later adopting application of the forte form, particularly when the corresponding reactions or improvements should fail to materialize as anticipated. In the event the Injeel-forte form should also fall short of achieving the desired therapeutic success, low single potencies are then to be applied.
For example, Anthracinum-Injeel in single potency D10 is several potencies lower than Anthracinum-Injeel forte, which contains the potency chord D15, D20, D30, D200. Bacterium coli in single potency D5 is one potency lower than Bacterium coli-Injeel forte, which applies for several other ”bacterial“ nosode preparations, e.g., also for Bacterium lactis aerogenes, Bacterium proteus, Bacterium pyocyaneus, and Brucella abortus Bang.
Higher potencies (single higher potencies) should only be employed when excessive reactions occur to the normal Injeel form of the corresponding nosode preparations. Thus, Variolinum in single potency D200 and/or D1000 and/or Vaccininum in single potency
D200 will be employed when excessive reactions to Variolinum-Injeel (D20, D30, D200) and/or to Vaccininum-Injeel (D20, D30, D200) occur once.
The following rule for treatment in general is particularly true in regard to nosode therapy: The higher potencies (D12, D30, etc.) are indicated for treating:
- increased irritability (Arsenic, Phosphate, Iodine or Chamomile Type)
- diathesis
- allergy and
- chronic disorders
The lower potencies (approximately D6/D8 and lower) are indicated in treatment of affections which are more or less acute:
- slow-reacting types of individuals (Sepia, Nux-vomica, Graphites, Silicea types)
- when organotropic action on a specific organ is desired (e.g., the tonsils: Tonsillarpfröpfe-Injeel forte and/or Tonsillitis Nosode-Injeel forte, each in potency chords D6, D10, D30 and D200).
Indications for higher potencies generally require relatively lengthy intervals of up to several weeks’ duration between applications.
Conversely, indications for lower potencies usually require only brief periods between applications, approximately 3 doses per week.
The recommended procedure is to commence administration by means of i.m., s.c. or i.d. injection (neural and/or acupuncture points); only in the event that this mode of application fails to evoke response may the corresponding nosode be administered i.v. in appropriate cases.
The application of the nosode Injeels during a progressive auto-sanguis therapy is advantageous. The nosodes should however always be applied during the last stage.
Note on dosage and potentization of nosodes in therapy of children
No essential difference exists between the dosage of nosode preparations and that of other homoeopathic agents in treating young patients, i.e., children receive a (somewhat) smaller dose than the adult patients.
Dosage (per application) for children:
0– 1 years of age approximately 0,3 ml 1– 6 years of age approximately 0,5 ml 6–12 years of age approximately 0,6 ml > 12 adult dosage For children, the lower potencies of D4 – D8 are administered at the beginning of therapy as well as in treatment of affections which are more or less acute; thus the same procedures are followed as for adults. Likewise, the higher potencies (approximately D12– D30) are used in both child and adult patients ensuing initial treatment with lower potencies (D4 – D8) and/or for therapy of chronic affections. Thus the same particulars apply for children in regard to potentization as they do in treatment of adults.
General
In their capacity as ”terrain remedies,” nosodes provide effective reinforcement for virtually every type of therapy. Nosodes frequently fulfil the role of a missing link in a series or chain of therapeutic reactions, whereby cure without the nosode is inconclusive or can be attained only under extreme difficulty. From a homotoxicological aspect, nosodes are chiefly applied in order to transform cellular phases into humoral phases, i.e., in order to achieve regressive vicariation. Nosodes are indicated in treatment of humoral phases as well, especially in cases which are in jeopardy of lapsing into a chronic condition such as in which there is impending danger of progressive vicariation.
Therapists working in the field of electro-acupuncture find the use of nosodes especially interesting due to the capabilities of such specialists to precisely determine the corresponding nosodes through the technique of medicinal testing. Thus therapy with nosodes is exceptionally effective in combining ”apparatus medicine” by means of the above-mentioned medicinal testing (bioelectric technique of drug determination), where appropriate, with the therapist’s ”eye for clinical diagnosis” or ”visual diagnosis.” Here, as always, the nosodes are to be administered according to symptomatic similarity, i.e., on the basis of the fundamental homoeopathic rules of similitude and employing the ”diagnostic aid” provided by the anamnesis, whereby any anamnestic, etiological similarity to a past, apparently cured illness is also taken into consideration. One should bear in mind in this respect that the extraordinarily good diagnostician and the excellent therapist is often recognizable by his or her ability to compile a skilful and accurate anamnesis.
-
Single Constituent Preparations and Classical Homeopathic Remedies
Single-constituent homoeopathic preparations
Available both in Injeel (Injection-remedy Heel) and in single-potency form, these homoeopathic single-remedy agents may be subcutaneously injected, i.m., s.c., i.d. (segment therapy) or i.v. All single-constituent preparations and Injeels may also be administered orally in water or tea (see chapter C, section 2, page 439), an attribute particularly suitable for treatment of infants and small children. Each ampoule of an Injeel comprises several potencies of the same basic remedy in parallel existence to one another within a potency chord.
The basic potency of an Injeel is generally D10 or D12, with equal parts of D30 and D200 as additional components. As a rule, Injeels of the ”forte” type contain equal parts of (D4), D6, D12, D30, D200 and possibly D1000. With the administration of a potency chord the organism is addressed on several hierarchical levels, namely on the organotropic level by the low potency, on the functiotropic level by the medium potency, and on the ”informative“ or ”mental“ level with the assistance of the higher potency.
Since, particularly during the course of regressive vicariations of chronic or severe illnesses of phases 4, 5 or even 6, considerable functional and informative errors occur in addition to the macroscopically detectable organic-structural errors, such potency chord preparations are also suited for the excretion of cellular illnesses due to the high potencies contained therein.
The principle of the potency chord is that any adverse reaction which may occur upon application of lower potencies of a medicinal agent can be mitigated and reduced through the simultaneous administration of higher potencies of the same medication (high-potency inverse effect). As a rule, treatment should always commence with simultaneous application of single-remedy Injeels, catalysts, and specialized preparations. The forte forms are to be administered in treatment of acute disease and illnesses which have become organically detectable.
Classical homoeopathic remedies
Anti-homotoxic medicine seldom requires – especially when the indication is obvious – homoeopathic single constituent remedies in single potencies. These single remedies are administered in terms of classical homoeopathy according to the simile principle. In anti- homotoxic medicine these single remedies are available as ampoules. Figure 7 shows an overview of the single remedies in single-potencies (ampoule form), which are available in addition to the single remedies in potency chords, nosodes, suis-organ preparations, etc.
D = X
-
Anti-homotoxic Preparations
Therapy with Anti-homotoxic Preparations from Heel
The Heel Company provides the following medications for use in anti-homotoxic therapy:
Combination preparations
composed of several potentised single substances (in low to higher potencies): Specialized preparations (e.g., Cralonin, Vertigoheel, Traumeel S, etc.) Homaccords (e.g., Aconitum-Homaccord)
Composita preparations (e.g., Echinacea compositum S)
Single-constituent homoeopathic preparations
as potency chords or as single potencies. Potency chords are labelled with the supplement ”Injeel“ or ”Injeel forte”; they contain high and higher potencies to calm possible initial reactions:
Classical homoeopathic preparations
Homoeopathically adjusted allopathic medications (e.g., Penicillin-Injeel) Catalysts (e.g., Ubichinon-Injeel) including those of the citric-acid cycle Nosodes (e.g., Sinusitis-Nosode-Injeel)
Suis-organ preparations (e.g., Cerebrum suis-Injeel)
The administration forms are injections, solutions, tablets, drops, nasal sprays, suppositories, and ointments.
Combination preparations
Specialized Preparations
Today, these specialized preparations are employed in practices of all types, regardless whether the practitioner is naturopathically oriented or not. These valuable medications (e.g., Vertigoheel, Traumeel S) also find application at university clinics and similar institutions. Figure 6 represents only a limited, subjective selection from the extensive assortment of specialized preparations available.
Fig. 6: Selection from the range of specialized preparations
Preparation Chief Indications Cralonin Geriatric heart, cardiac neurosis Engystol N Influenza, febrile virus infections Gripp-Heel Influenzal infections Lymphomyosot Lymphoedema, tonsillitis, increased susceptibility to infection Rheuma-Heel Non-articular rheumatism syndrome Spascupreel Colic, myogeloisis Spigelon Headache Traumeel S Arthritis, arthrosis, sports injuries Vertigoheel Dizziness of various origius Viburcol Fever, minor infection, excitation Ypsiloheel Vegetative dystonia, globus hystericus Zeel/Zeel comp. Arthrosis, polyathrosis Homaccords
Homaccords are preparations which contain one or several active substances in respective potency chords. Usually a low potency is combined with a medium potency and a higher potency. The background of this potency combination is the nearly 100 year old therapeutic experience that the simultaneous administration of low, medium, and higher potencies causes a reduction of the initial aggravation. As is known, initial aggravations occur particularly often during the administration of higher potencies given individually.
Homaccords are available both as attenuations for oral administration as well as in ampoule form for subcutaneous injection. This multipotent form – among other applications – is particularly appropriate for treating chronic illnesses.
In the ampoule form of the Homaccords, the individual constituents’ potency-levels are generally two to three stages higher than those found in the drops. These highly- potentised elements exert a subduing effect on any possible initial reactions, hence cases displaying initial aggravation are a rarity.
Composita Preparations
In order to obtain a preparation which is highly effective on the one hand, yet low in risk and side effects on the other, the expedient solution was to unite a number of various homoeopathic single-remedy medications, homoeopathically adjusted allopathic medications (see below), intermediary catalysts (see below) and – in certain cases – suis- organ preparations (see below) within one single combination preparation.
Through the multiplicity of constituents within Composita preparations, a broad, in-depth therapeutic effect is achieved. The basis for this are the various points of action at which the constituent medications develop their efficacy. The basic principle of the Composita preparations will be explained vicariously with the example of Euphorbium compositum Nasal Spray. This nasal spray preparation contains as classical homoeopathic botanical constituents Euphorbium, Pulsatilla, and Luffa operculata, further the anorganic-chemical, classical homoeopathic substances Mercurius bijodatus, Argentum nitricum, and Hepar sulfuris, the nosode Sinusitis-Nosode and the suis-organ preparation Mucosa nasalis suis. The constituent ”Euphorbium,“ which lends its name to the preparation, demonstrates clear relations to illnesses of the upper respiratory tract in its drug picture. The organotropically implemented low potency of Euphorbium resinifera is supported by the constituents Pulsatilla, Luffa, Mercurius bijodatus, and Argentum nitricum, which contain in their remedy picture the symptomatology of catarrhal inflammatory processes of the upper respiratory tract according to the Materia Medica Homoeopathica.
From a therapeutic viewpoint, the purpose of the Sinusitis-Nosode is to treat the illness underlying the chronic sinusitis etiologically (phase 3, deposition), which has settled in the area of the upper respiratory tract. It accomplishes this by reactivation based on the isopathic therapy principle through excretion via the excretion phase. The homoeopathically adjusted organ extract Mucosa nasalis suis basically acts on the mucous membrane region of the upper respiratory tract (homologous animal tissue; Schmid1), Reinhart2)). All of the applied active substances occur in potencies between D2 and D13, in other words, these are active substances in the so-called low potency and medium potency range; potencies of these ranges basically act organotropically and functiotropically according to the homoeopathic view. The therapy of chronic sinusitis is possible particularly through the nosode because nosode preparations exercise a positive effect especially on chronic processes and may reactivate them. In terms of anti- homotoxic therapy a chronic illness already in a matrix phase (phase 3 or 4) is re-activated in terms of a regressive vicariation according to Reckeweg and is returned to the inflammatory phase 2. The organotropically acting, classical homoeopathic remedies Pulsatilla, Hepar sulfuris, Mercurius bijodatus, Euphorbium, and Luffa can then fully develop their efficacy in this activated inflammatory phase.
Thus, this rational basic principle of uniting substances of diverse efficacies in one compositum preparation provides a new, therapeutically promising access to the treatment of chronic illnesses. The following reflections should elucidate this more closely:
- Because chronic illnesses usually progress in syndromes and unite various causes into one diagnosable clinical syndrome, a medicinal therapy with the assistance of one single substance is seldom promising, as experience shows. By classifying the diagnosed disease into the Six-Phase-Table of Homotoxicology, the selection of the respective homoeopathic remedies for diseases of the matrix phase as well as of the degeneration and the dedifferentiation (neoplasm) phase, that is, basically for cellular diseases to the right of the Biological Division, need not be limited solely to the classical homoeopathic remedies from the botanical, mineral, and animal kingdoms.
- In combination with nosode preparations, suis-organ constituents, and catalysts, the therapist gains the possibility to treat further progressed cellular phases to the right of the Biological Division, because, by removing the enzyme blockades though the catalysts or through an isotherapeutic ”massive nosode dose“ as well as through the suis-organ preparations, a regression of the disease in terms of regressive vicariation is activated.
- As soon as a regressive vicariation into a humoral phase has taken place through the penetrating nosodes, catalysts, and suis-organ extracts, the organotropic, classical homoeopathic remedies can effectively induce the healing of the developing inflammatory phase.
- The potency D8 of the organ constituent Mucosa nasalis lies in the so-called substitutive range. To this extent, this range is comparable to the organotropic range of the classical homoeopathic lower potencies (Schmid)1) and explains the direct action of these organ preparations on the homologous human tissue. With potencies up to the order of magnitude of approximately D12, a material action of these active substance molecules on endogenic function bearers such as enzymes, membrane receptors, and cellular structures of immunological cells or organ cells is still given, according to present conceptions, through the material presence of active substance molecules or their fragments (Heine).2)
- Since, according to Paracelsus, every poison is its own antidote, the dose determines whether a substance has a poisonous or a healing effect for the patient. The potentised nosode can also be designated as its own antidote. The no-sode – in this case the sinusitis nosode – is extracted from a pathological secretion of a sinusitis patient. This effluence contains the complete information of the illness ”sinusitis.“ Through homoeopathic preparation and potent zing to D13 in the present case, a direct toxic effect is excluded, on the contrary, the specific antidote effect of the nosode in terms of the Arndt-Schulz inversion law is released through the potent zing.
Moreover, potentised homoeopathic substances comply fully with the Arndt-Schulz law, which generally purports that weak stimuli, e.g., potentised homoeopathic substances, exercise a stimulative effect. This statement is basically supported by the modern hormesis research in toxicology, which demonstrates that a highly toxic substance such as mercuric salt, administered in the milligram range, exercises a strong toxic effect. However, after potent zing to D8 and higher, it demonstrates a stimulative effect which practically reverses the original toxic effect. The German pharmacologist Prof. Schulz was already able to repeatedly verify the ”bi-phasal“ effect of active substances in his experiments 100 years ago.
This means that a substance in a certain dose range exercises a toxic effect and loses this toxic effect after further dilution (potent zing). After potent zing a new, therapeutically useful effect reveals itself which represents practically the opposite of the original toxic effect.
Such reversals of effect and phasal effects of highly diluted toxins, e.g., anorganic salts from heavy metals and organic substances were also described by T.D. Luckey3) and E.J. Calabrese4) in recent overviews.
References
- Schmid, F. Anti-homotoxische Medizin, Band I: Grundlagen, Klinik, Praxis; Aurelia-Verlag, Baden-Baden, 1. Aufl., 1996
- Heine, H. Lehrbuch der biologischen Medizin – Grundlagen und Systematik; Hippokrates Verlag, Stuttgart, 2. Aufl., 1997
- Luckey, T.D. Hormology with Inorganic Compounds. In: Luckey T.D., Vleingopal B.Hutcheson D., editors. Heavy metal – toxicity, safety and hormology. Stuttgart, New York, San Francisco, London, Georg-Thieme-Verlag, 1975; 81-103
- Calabrese, E. J. Biological Effects of Low Lever Exposures to Chemicals and Radiation; Lewis Publishers, Inc., Michigan, 1991
-
Medicinal-therapeutical Mechanism of Action of
2.1 The difference between anti-homotoxic preparations and single homoeopathic remedies
Whereas the classically treating, homoeopathic therapist exclusively applies so-called single-constituent remedies, whose constituents are potentized according to the defined production rules of the homoeopathic pharmacopoeia and whose application is conducted after anamnesis and subsequent repertorization according to the Simile Principle, anti- homotoxic preparations are usually implemented based on the indica-tion. The anti- homotoxic preparations are usually composed of combinations of homoeopathic substances, manufactured according to the regulations of the official German Homoeopathic Pharmacopoeia (HAB 1978), and are homoeopathic remedies according to the legal definition of the EU guideline 92/73 EC.
Unlike single homoeopathic remedies, it is essential during the therapeutic implementation of anti-homotoxic preparations that these remedies are applied based on the measures of Homotoxicology according to Reckeweg. In particular this means that the physician first defines the current location of the patient as indicated on the Six-Phase-Table of Homotoxicology.
Due to the phasal course of diseases the physician must pay attention to so-called vicariation effects, i.e., the shifting of a disease from one phase into another. The therapeutic goal is to shift the disease from a phase to the right of the Biological Division (phases 4 to 6) into a phase to the left of the Biological Division (phases 1 to 3). To achieve this the excretion of homotoxins must be initiated with the corresponding anti- homotoxic preparations.
Due to the high complexity of chronic diseases, it is essential for the success of anti- homotoxic therapy to implement the anti-homotoxic preparations in accordance with the phases. The rule of thumb may apply thereby that in particular the so-called combination preparations are indicated for diseases in the matrix phases 3 and 4 as well as in the degeneration and dedifferentiation (neoplasm) phases. This applies essentially because, in addition to the specific classical homoeopathic active agent, further anti-homotoxic active agents such as potentized suis-organ extracts, catalysts, nosodes, and, in several cases, also the homoeopathically adjusted allopathic medications are contained in these preparations. As practice has shown, well selected single homoeopathic remedies are often not able to shift a disease from the cellular phases 4 or 5 into a regressive vicariation unless certain enzyme defects or blockades on the cellular level are previously removed by anti-homotoxic agents such as catalysts, suis-organ components, nosodes, and homoeopathically adjusted allopathic medications. The action of the indicated simile occurs only after the removal of the blockades because the homoeopathic single remedy requires a terrain which is at least still partly responsive to stimulants. Reaction blockades must be removed with other strategies such as the anti-homotoxic excretion, the progressive auto-sanguis-therapy, neural therapy, and dietetics.
Experience has shown that well selected single remedies + Injeels/forte from the area of the catalysts, nosodes, and suis-organs or corresponding combinations, in particular the so-called Compositum preparations are suitable to achieve ”regressive“ vicariation. If, however, a regressive vicariation effect has occurred and the secondary or tertiary disease (locum disease) has regressed into phase 2, then the single remedies or the customary specialties of the anti-homotoxic preparations, which contain combinations of single remedies, can be successfully applied.
To achieve the successful application of the anti-homotoxic preparations, the following details must be noted from the above explanations:
- The definition of the phase which the disease is in.
- The recording of vicariation effects.
- The excretion of homotoxins.
- The anti-homotoxic or homoeopathic treatment of the disease arisen after vica-riation into the excretion phase.

2.3 The treatment of diseases to the right of the Biological Division with anti-homo-toxic preparations
The phases to the right of the Biological Division possess the following common properties:
- They have gone through a longer development time, that is the diseases have assumed a chronic nature.
- As a result of the chronicity, intracellular, structural damages have, as a rule, occurred on the organelles of the cells.
- The structural damages are frequently due to blockades of physiological meta-bolical process chains (enzyme blockades).
- The matrix is severely altered in its functionality through deposits of metabolites (= homotoxins) and through the frequently accompanying acidosis.
- The alteration of the matrix impacts on the immunological reactions within the matrix (immunotoxically and paradoxically proceeding reactions).
- The proper supply of neighbouring parenchyma cells with the nutrients trans-ported via the blood capillaries is severely altered or limited (disorder of the transportation function of the matrix).
Together with the alteration of the matrix and the physiological reaction of the matrix the removal of contaminants and metabolites is impeded, resulting in the retoxifying action of these waste products (homotoxins) on the parenchyma cells to be supplied.
Based on the above listed alterations particularly in the matrix, the general anti-homotoxic strategy aims to repair these damages for diseases to the right of the Biological Division by:
- Reduction of further contaminant supply e.g., by changing the diet.
- Unblocking of enzyme systems particularly in the metabolically active organs such as the liver and kidneys as well as the intestinal tract and the lungs with the aid of the catalyst preparations.
- Elimination of the tissue acidosis, e.g., through an alkalic diet.
- Drainage of the matrix via the diverse detoxification techniques such as lymph drainage, physical therapy (sauna), administration of corresponding homoeo-pathic preparations (e.g., Lymphomyosot).
- Therapeutic restitution of damaged intracellular structures via suitable anti- homotoxic preparations (e.g., suis-organ preparations).
For the drainage of the matrix it is recommended to administer nosodes in addition to lymphatic remedies because the nosode as an isotherapeutic remedy causes a highly specified stimulus for the alteration of the toxic situation. Nosodes are, as is known, therapeutic remedies of the terrain and possess the ability to ”remind“ the body specifically of the ”similar“ or comparable general toxic situation of the diseases wich they represent.
In addition it may be required for the treatment of a retoxifying action caused by frequent intake of strongly effective allopathic medications to offer the corresponding homoeopathically adjusted allopathic medication to the sick organism. By homoeopathically adjusting the allopathic medication, generally in the D6 potency and higher, a reversal of the toxic action of this medication is induced. The Arndt-Schulz law and/or the effect of hormesis provide a logical scientific explanation for this retroactive effect.
The unblocking of enzymes or metabolic chains is effectively achieved by the administration of anti-homotoxic catalyst preparations such as Coenzyme compositum in alternation with Ubichinon compositum. Both preparations contain a significant combination of vitamins and co-enzymes as well as intermediary products of metabolic cycles providing energy in the homoeopathic dilution from D6. According to Schmid1) these preparations act on the molecular level on the mitochondria and assist the organism to regulate the intracellular, energy-supplying processes once again. The potencies between D6 and D10 are substitutive and can reactivate metabolic dysfunctions in energy- supplying cycles by substitution.
Because every severe disease, which no longer possesses any self-healing tendencies, is coupled to dysfunction on the level of energy-supplying processes, a concomitant, possibly intermittent administration of these preparations is indicated in all cases, as frequently confirmed successfully both in human medicine and in veterinary medicine.
The two catalyst preparations ( Coenzyme compositum and Ubichinon compositum) can be significantly supplemented by the administration of a trace element compound such as Molybdän compositum. In this compound, important trace elements such as molybdenum, zinc, iron, cobalt, cerium, manganese, copper, nickel, and rubidium are combined with sulphur and phosphorus which both possess a strongly stimulative effect particularly on mucous membranes and tissue cells and which belong to the so-called reaction remedies in homoeopathy. The above-mentioned trace elements are present as salts in lower potencies between D3 and D8. In these ranges, these trace elements no longer have toxic effects, but have a purely stimulative and/or a substitutive effect. These elements catalyze several enzyme-dependent reactions. As is well known, particularly molybdenum, copper, nickel, zinc, manganese, and cobalt are elements which are essential for certain enzyme complexes, that is, these enzyme complexes cannot function without them.
It can be said in summary that the Compositum preparations containing catalysts, minerals, and trace elements are indicated for all chronic diseases connected with energy deficits such as chronic fatigue syndrome or for diseases caused by old age.
2.2 The treatment of diseases to the left of the Biological Division with anti-homo-toxic preparations
The treatment of diseases of phases 1 to 3 can be conducted with relatively nonspecific homoeopathic substances. Nonspecific signifies in this case that the point of attack of the preparation does not concentrate on a specific, e.g., degenerately damaged organ, but that it exercises an effect upon the whole organism particularly via the blood and lymph system.
Practice has shown thereby that such diseases of the humoral phase, and particularly of the deposition phase (phase 3) are very effectively treated with the progressive auto- sanguis therapy, that is, an autologous blood nosode combined with specialties and/or reaction remedies which do not belong to the Compositum preparations. Typical representatives of these preparations are, for example, nonspecifically stimulating preparations for all infectious diseases such as Gripp-Heel, Engystol or Traumeel S. The effect of these preparations is effectively amplified by the progressive auto-sanguis treatment because an additional immunological stimulus is exercised on the matrix by this autologous blood nosode.
The Injeels of the single homoeopathic substances also belong in the treatment of diseases of the humoral phase because the advantage of the combination of low and high potencies is that they possess a quite conservative therapeutic efficacy usually progressing without initial aggravation.
It can be presupposed for all diseases of the humoral phase that the intracellular structures are still intact and that enzyme blockades or cellular structure defects have not yet occurred. For this reason, the organism can be stimulated directly by the homoeopathic simile in terms of an antidote and this effect may possibly be amplified by the analogous blood nosode as well. The homoeopathic drug picture is defined, as is well known, based on the healthy test person who does not have a cellular illness.
In the third phase, the deposition phase, the homotoxin is simply encapsulated and taken out of circulation, so to speak. This phase always occurs when the homotoxins can no longer be degraded by the body in the reaction phase.
During the deposition phase the condensed homotoxins are deposited without causing structural alterations of the matrix and/or functional impairments to it. As long as the physiological filtering and protection functions can be performed by the matrix, the regular supply of the surrounding parenchyma cells and tissue is guaranteed. The situation only changes dramatically when the Biological Division is crossed, when the endogenic structure of the matrix is so burdened by more and more condensed, deposited homotoxins that it can no longer perform its filtering and protection functions. In such a case the homotoxins enter the tissue cells where they cause cellular, structural alterations in cell organelles such as mitochondria or nuclei.
2.4 The course of therapy
By introducing the vicariation principle into anti-homotoxic therapy Reckeweg pointed out the dynamics of every disease and/or recovery process. The interrelations which exist between a bio-system and the damaging homotoxins vary continuously during an illness and during the recovery process. The purposeful, self-regulatory forces of the organism usually are retained during illnesses up to and including the 3rd phase of the Six-Phase Table of Homotoxicology. In contrast, after the Biological Division is crossed, from phase 4 onward, self-regulation and self-recovery is practically no longer possible for the organism. In this case, a therapeutic-medicinal treatment is required to achieve recovery.
Following regressive vicariation, a disease often enters either phase 2 or 3. This usually requires the change of the anti-homotoxic preparation because in phase 2 the symptomatically indicated acute remedy is usually necessary. In phases 2 and 3, which belong to the humoral phases, the self-regulatory capacity of the organism is still present, so that only stimulative medication is required to initiate inflammatory mechanisms, particularly in the matrix. Usually the excretion of the disease occurs via the skin or the mucous membranes. Increased perspiration, sputum, strong formation of urine, light diarrhea, and fever are welcome signs of a shift out of the cellular disease phases which indicates an improvement of the basic illness. In the acute phases 1 and 2, Compositum preparations as described previously are generally no longer required but instead, preparations such as Traumeel or certain Homaccords or single-remedy Injeels are preferable.
2.5 The modes of application of anti-homotoxic preparations
Anti-homotoxic preparations can be applied orally, parenterally, or locally/externally. Particularly for easily located complaints, a combination of oral with local measures, e.g., for the treatment of injuries or rheumatic diseases, is recommended. In addition, a segmental, parenteral treatment of certain areas of the body via subcutaneous or intracutaneous infiltration is a frequently practiced procedure for the treatment of painful diseases of the locomotor system. The most wide-spread mode of application is – as generally also for homoeopathic preparations – the systematic oral application via tablets or drops and/or the application of suppositories for children.
If desired, ampoules can be administered orally instead of parenterally. This application is particularly recommended when alcoholic drops should not be used for small children or alcoholic patients.
The application of injections is polymorphic; it includes the intravenous, intramuscular, subcutaneous, and intracutaneous application, and also the segmental, the periarticular as well as – in certain cases – the intra-articular application. The parenteral application is advisable as a periarticular or subcutaneous injection especially for joint complaints and easily located pains. Through infiltration of anti-homotoxic preparations in combination with neurotherapeutical substances such as Procaine or Xylocaine freedom of complaint can be achieved quickly and without complications. Finally, the application in acupuncture or trigger points is an effective mode of application for anti-homotoxic preparations (Homoeosiniatrical Application). 2, 3, 4)
2.6 References
- Schmid, F. Anti-homotoxische Medizin, Band I: Grundlagen, Klinik, Praxis; Aurelia- Verlag, Baden-Baden, 1. Aufl., 1996.
- Skribot, E.W. Anwendung von Homöopathika in die homöosiniatrischen Aku- punkturpunkte; Biologische Medizin, Band 9, Heft 2, 1980; 51-63.
- Ebert, H. Homöosiniatrie, Haug-Verlag, Heidelberg, 1992.
- De la Fuye, R., Schmidt, H. Die moderne Akupunktur; Hippokrates-Verlag, Stuttgart, 1952.
-
Homotoxicology
Classical homeopathy according to Hahnemann (1811) orients itself based on the so-called ‘drug picture’ to determine the appropriate remedy. It claims that symptoms of disease behave reciprocally towards those symptoms which the healthy test person develops after the intake of a mother tincture or a diluted substance (potency.) The principle of action which can be derived thereof is known as the Simile Principle (Similia similibus curentur = Likes may be cured by likes.) The clinical syndrome occurring in a patient can be overcome by an artificially induced, similar disease. The Aequalia Principle (Isopathy = the condition may be healed by the causative substance) can also be applied with potentised allopathic substances or partly with nosode preparations in anti-homotoxic medicine and/or with vaccines in conventional medicine.
Classical homoeopathy works with single remedies which are only partly truly single- constituent remedies, (e.g., sulphur, mercury, arsenic, etc.), or which are otherwise botanical extractions containing a highly complex mixture of numerous constituents. Repertories (lists of symptoms produced by drugs) facilitate the selection of the most appropriate remedy in homoeopathy.
Anti-homotoxic medicine usually pursues an indication-oriented approach. The anti- homotoxic remedies predominantly represent mixtures of substances of low to middle potencies. Through practical application in homoeopathy it became obvious that the use of concentrated or poisonous tinctures could damage the patient and that, therefore, they could only be used in homoeopathic dilutions, i.e., potencies. This practice was scientifically supported by Rudolf Arndt (psychiatrist, 1835-1900) and Hugo Schulz (pharmacologist, 1853- 1932) through a quantitative differentiation of the medicinal effect on bio-systems and still applies as the Arndt-Schulz Principle. It states:
- weak stimuli stimulate the life functions (retro-action of homoeopathic preparations)
- moderately strong stimuli accelerate them
- strong stimuli act as inhibitors
- the strongest stimuli suspend the life functions
Since several tissue-incompatible substances are usually involved during the development of a disease, the simultaneous use of several potentised ”antitoxins“, as present in the anti- homotoxic preparations, is justified.
Against the background of the conflicting medicinal and therapeutic concepts promulgated in humoral pathology, cellular pathology, molecular pathology, and related fields including modern cybernetics, the German physician Dr. Hans-Heinrich Reckeweg formulated Homotoxicology in 1952. This conception was developed from homoeopathy for the purpose of providing a holistic perspective on the synthesis of medical science.
Reckeweg formulated an essential tenet of Homotoxicology, as follows:
”According to Homotoxicology all of those processes, syndromes, and manifestations, which we designate as diseases, are the expression thereof that the body is combating poisons and that it wants to neutralize and excrete these poisons. The body either wins or loses the fight thereby. Those processes, which we designate as diseases, are always biological, that is natural teleological processes, which serve poison defence and detoxification.“
Referring to conventional medical indications connects anti-homotoxic medicine with allopathy, while therapy with potentised substances unites it to homoeopathy. Anti-homotoxic medicine is the connecting link between allopathic medicine and homoeopathy.
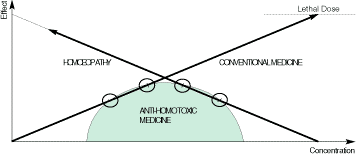
Fig. 1
Conventional medicine:
The higher the concentration, the stronger the effect (dose-effect relation; increase of side effects).
Homoeopathy:
Increase of the effect with decreasing concentration (effect optimum not definable). Anti-homotoxic medicine:
Connecting link between conventional medicine and homoeopathy.
- Fundamental principles of Homotoxicology
1.1.1 Homotoxins
Homotoxins are all of those substances (chemical/ biochemical) and non-material influences (physical, psychical), which can cause ill health in humans. Their appearance results in regulation disorders in the organism. Every illness is due therefore to the effects of homotoxins. Homotoxins can be introduced from the exterior (exogenic homotoxins) or originate in the body itself (endogenic homotoxins).
1.1.2 Homotoxons
These are understood as chemical reaction products from compounds of homotoxins with each other or with other substances (e.g., products of metabolism) which neutralize the poisonous property of the homotoxins. The best example thereof is the liver, in whose cells homotoxins and metabolic products are united to detoxify the organism.
1.1.3 Retoxins
Deposits of homotoxins with endogenic substances, which cannot be eliminated via excretion or irritation, are designated as ”residual poisons“ (retoxins). The most important example thereof is the non-enzymatic glucosilisation of tissues and cell surfaces in case of glucose excess, as with, among others, latent diabetes mellitus.
1.1.4 Homotoxicosis – The Concept of Disease in Homotoxicology
Homotoxicosis is a non-physiological condition which arises after reaction of a homotoxin on cells and tissues. A homotoxicosis occurs as a humoral or cellular appearance and can be followed by morphological changes on tissues. The homotoxicosis is named after the homotoxin which triggers it. The homotoxicosis leads to defensive measures of the organism whose goal is to eliminate the homotoxins and to restore the physiological conditions when possible.
1.1.5 The Ground Regulation
This refers to the local regulation possibilities of the ground system along with its superimposed nervous, hormonal, and humoral regulation systems. The ground system is composed of the ground substance plus cellular, humoral, and nervous components. The ground substance (extracellular matrix) is formed of highly polymerised sugars (proteoglycans and glycosaminoglycans) plus structural and meshing glycoproteins.
1.1.6 The Phase theory
The Six-Phase-Table illustrates the chronological courses of various symptoms of a disease within the framework of the ground regulation. The single phases are transient into each other and demonstrate typical phasal indicating signs. The Six- Phase-Table is subdivided into three sections (humoral phases, matrix phases, cellular phases), each of which is subdivided into 2 phases. Two phases are allocated to the excretion principle (phases 1 + 2), the deposition principle (phases 3 + 4), and the degeneration and/or deterioration principle (phases 5 + 6). The Biological Division runs within the matrix phases.
Fig. 2: The Six-Phase-Table
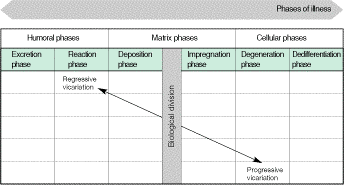
- The humoral phases
In the humoral phases the intracellular systems are not disturbed. The defence system is intact and can excrete the homotoxins via various paths.
- Excretion This phase contains manifestations of increased physiolo- phase gical excretion mechanisms.
- Reaction Illnesses of this phase are marked by an exudative inflam- phase mation, which enables an accelerated excretion of toxins
from the body.
B) The matrix phases
In these phases the homotoxins are deposited at first in the mesh of the extracellular matrix. During the further course its structural components as well as functions are al-tered. In case of continuing illness increasing stress and damage of the intracellular structures result.
- Deposition In this phase the excretion mechanisms of the body are phase overworked and toxins are deposited in the matrix.
This phase often progresses with few symptoms.
- Impregnation Diseases in this phase are characterized by the presence phase of toxins which become a part of the connective tissue
and the matrix, along with changes in the structural com- ponents as well as their functions. The typically increasingly severe symptoms and signs of this phase demonstrate damage of the organ cells.
C) The cellular phases
During the cellular phases of a disease, cell systems are increasingly destroyed. The defence system is no longer able to excrete the toxins out of the cells or out of the matrix by virtue of its own strength. Typical for these phases is the so-called regulation rigidity.
- Degeneration During this phase, courses of disease cause serious dam- phase age, and destruction of larger cell groups of an organ
takes place.
- Dedifferentiation Diseases of this phase are characterized by the devel- (neoplasm) opment of undifferentiated, non-specialized cell forms. phase Malignant diseases stand at the end of this phase.
1.1.7 Biological Division
The Biological Division refers to the imaginary boundary between the deposition and impregnation phases. It demarcates the pure deposition in the matrix from the integration of toxins into its structural components. Whereas a simple excretion of the toxins is possible during the deposition phase, structural and functional changes are found in the impregnation phase. Thus the spontaneous endogenic excretion of the homotoxins is impeded.
1.1.8 Vicariation
The term ”vicariation“ refers to the transition of the indicating signs of an illness within one phase to another organ system, or the change of the fundamental symptoms and signs into another phase, with or without a change of the organ system.
Progressive vicariation: Progressive vicariation refers to an aggravation of the total symptoms and signs of illness.
Regressive vicariation: Regressive vicariation refers to an improvement of the total symptoms and signs of an illness.
1.2 The principles of action of anti-homotoxic medicine
The different components of the anti-homotoxic preparations activate the defence system of the body:
Fig. 3: Functional circle of the anti-homotoxic therapy
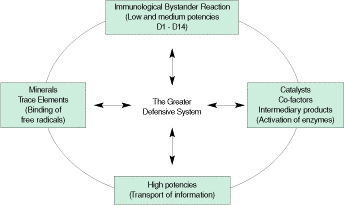
The immune system with its memory and regulation systems can be compared to the spiritual-mental self, the ego. The deposition phase, and more frequently the impregnation phase, is characterized by immunological processes such as chronic inflammations and auto- aggression. The humoral area (via immunoglobulins from B-lymphocytes) and the cellular area (T-cells, granulocytes, macrophages) still counterbal-ance each other in this case. A regressive vicariation is still possible in these matrix phases.
Herein lies a great opportunity for anti-homotoxic medicine. The immunological bystander reaction represents a theory of anti-homotoxic therapy for inflammatory illnesses. It is based on low dose antigen reactions particularly of substance combinations in the range of D1 to D12, with D4 to D8 appearing to be the most favourable (Heine, 1997b). The bystander effect cannot be triggered at higher potencies, however experience shows that higher potencies as well as trace elements and intermediary catalysts are able to stimulate the ground regulation. (Functional circle of the anti-homotoxic therapy; Fig. 3; Heine, 1997a.) It is significant that, for the potency ranges D3 to D12, a considerable difference exists in the activation of specific enzyme systems compared to substances conventionally diluted in the same concentration. The dose-action relationship of potentised substances compared to diluted substances demonstrates thereby a non-linear relationship (Hoariest and Dittmann, 1997).
Ground regulation system
Every organism requires energy to maintain its vital functions which must be continuously provided by the metabolism. Therefore, disorders of the energy metabolism impair the energy supply which is controlled by the endogenic regulation. The organism is an energetically open system for which suitable energy (in the form of food) must be supplied, and unsuitable energy must be evacuated. In this manner an unstable state of order can be maintained, far from a thermodynamic balance, for a longer period of time (”life-span“). All reactions of the organism proceed at relatively low temperatures in the aqueous milieu, therefore they must be accelerated, i.e., catalysed. The prerequisite for an effective catalysis is suitable substrates between and in the cells. Be-cause the extracellular space is located in front of the cells, the cells can only react as they have been informed via the extracellular space. The dynamic structure of the extracellular space and its regulation (”Ground regulation“) have therefore a decisive impact on the effectiveness of extracellular and intracellular catalysts. This depends on the structure of the ground substance (extracellular matrix and/or matrix). It forms in all cells and cell groups a molecular sieve of matrix components such as highly polymerised sugar protein complexes and sugar complexes (proteoglycans-glycosaminoglycans, PG/GAGs), structural proteins (collagen, elastin) and meshing glycoproteins (e.g., fibronectin) (see Figure 4). The PG/GAGs are electro-negatively charged and are therefore able to bind water and exchange ions as well. They are therefore the guarantors for isoiony, isoosmy, and isotony in the matrix.
Fig. 4: Diagram of the ground regulation
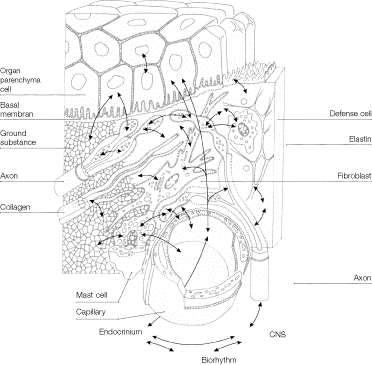
Reciprocal relationships (arrows) between capillary system (capillaries, lymph vessels), ground substance, terminal autonomic axons, connective tissue cells (mast cells, defence cells, fibroblasts etc.) and parenchyma cells. Epithelial and endothelial cell groups rest on a basal membrane which mediates to the ground substance. Every cell surface carries a glycoprotein and glycolipid film connected to the ground substance (dotted line), to which the histocompatibility complexes (MHC) also belong. The ground substance is connected to the endocrine system via the capillary system and via the axons to the central nervous system. The fibroblast is the metabolically active centre. (Heine 1997b)8)
The connection to the central nervous system is conducted via the autonomic nerve fibres blindly ending in the matrix. The connection to the system of endocrine glands (pituitary gland, thyroid gland, suprarenal gland, etc.) is conducted via the capillary system which permeates the matrix. Both systems are connected to each other in the brainstem and to superimposed centres of the brain (Fig. 4). In this manner the matrix is regulated not only on site but also under the influence of superimposed control areas. The regulation centre in the matrix is the fibroblast (corresponding to the glia cell in the central nervous system). It reacts immediately to all incoming information (hormones, neural substances, metabolites, catabolites, pH-value changes etc.) with a synthesis of matrix components suited to the situation. It does not differentiate thereby between ”good“ or ”bad“ information. In this manner every surplus or deficit can lead in certain circumstances to detrimental consequences for the total system depending individually on a circulus vitiosus (vicious circle).
It is important to note that due to the sieve-like as well as connective properties of the PG/GAGs, the danger of slagging of the matrix also exists through the development of a latent tissue acidity, increase of free radicals, and the activation of the proteolytic system turning into a pro-inflammatory situation. Ultimately, damage of all humoral and cellular elements may arise progressing at first from persistent feelings of ill health to chronic diseases and malignant processes. (See 1.1.6, page 11; summary in Heine 1997a.)7)
Immunological Bystander Reaction
Whether administered orally, as aerosol, nasally, i.v., s.c. or i.m., the anti-homotoxic preparations are either directly confronted non-specifically with the macrophages/monocytes or the substances are offered to them by lymphocytes patrolling the mucosa epithelia after superficial contact. After phagocytosis the macrophages return an amino acid motive (9 to 15 amino acids) of the substances to its surface. There they are bound to the MHCI complex (histocompatibility antigens) (Fig. 4). Thus the motives for yet undetermined (”naive“) lymphocytes (Th0) become recognizable. They accept the motives and convert themselves thereby into regulatory Th3-cells. Afterwards they wander via the lymph vessels into the nearest lymphatic node and form _motivated“ cell clones which enter the bloodstream via the post-capillary venulae and are distributed throughout the whole organism via the circulation. In dysregulatory areas, in particular inflammatory regions, the Th3-cells are chemotactically attracted (complement factors, chemokines etc.). According to their motives they can recognize inflammatory lymphocytes (T4-cells and their subpopulations T-Helper1- and T- Helper2 lymphocytes). A similarity of the motives (the Simile Principle of anti-homotoxic medicine!) suffices thereby to stimulate Th3-cells to secrete the anti-inflammatory cytokines TGF-b (tissue growth factor-beta) and to a slight degree interleukin-4 and -10. TGF-b is the most potent anti-inflammatory cytokine in the body. It suppresses the T4- and its helper cells. The Th2-cells support thereby their own inactivation through the release of IL-4 and IL-10
through which TGF-b is considerably strengthened in its anti-inflammatory function (Fig. 4). Simultaneously the B-lymphocytes are stimulated to synthesize immunoglobulins.
It remains to be noted that the immunological bystander reaction can only proceed in the low dose antigen range (ca. 1 µg to maximally 1 g per day and body weight).
[An excellent overview of the literature on the phenomenon of the low dose antigen reactions (”Bystander Suppression“) can be found in Weiner L, Meyer F. Oral tolerance: Mechanisms and Applications. Ann New York Acad Sci 1996; 778: 1-418.]
As demonstrated by Carvalho and Vaz (Scand. Journal Immunology 1996; 6: 13-18) in animal experiments, the injection of a tolerated antigen, e.g., endogenic fibrinogens is not immunologically neutral: A previously stimulated bystander reaction is possibly amplified thereby! The authors also explain this with the action of suppressive cyto kines from lymphocytes. These findings fit with the progressive auto-sanguis therapy according to Reckeweg.
Because the number of antigens is not known during inflammatory processes, it is very advantageous to offer a greater number of motives, as is customary in anti-homotoxic medicine, to approach an inflammatory process immunologically from several sides. (Fig. 5). The bystander reaction can be supported thereby by the auto-sanguis therapy according to Reckeweg. Thus, anti-homotoxic medicine offers great advantages because:
- it is not necessary to know the specific antigen in order to treat an illness of a specific organ, as similarity is sufficient (see Brandtzaeg, 1996),
- an adequate combination of low dose antigens must exist (D1 to approximately D14) to attain a corresponding bystander reaction,
- a circulating antigen blood level need not be provable (Weiner et al., 1994),
- individual differences occur in the reaction to various epitopes of the regulatory lymphocytes (Friedman and Weiner, 1994; Weiner et al., 1994),
- the bystander reaction can obviously also be triggered regardless of the method of application (oral, nasal, s.c., i.m.)
(Al-Sabbagh et al., 1996; Carvalho and Vaz, 1996, Chen et al., 1996),
- the bystander reaction regulates dysfunctions and does not block them,
- a function cycle of anti-homotoxic therapy exists, which acts in a regulatory manner in the ground system.
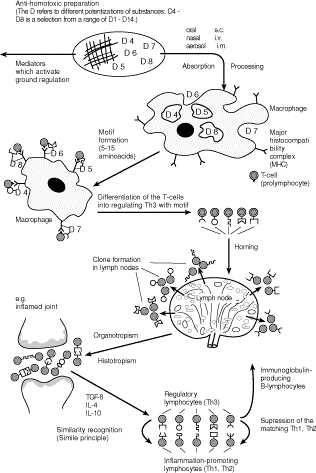
Fig. 5: The immunological bystander reaction as a principle of action of anti-homotoxic medicine
A D1-D14 potency of an anti-homotoxic preparation contains sufficient substance quantities to stimulate macrophages to form antigen motives after application (top). This is the prerequisite for the formation of regulatory lymphocytes (th3) (middle row). Th3 cells find chemotactically phlogogenic lymphocytes (t4, Th1, Th2) with similar antigen motives and suppress these by releasing TGF-b (bottem). (Heine 1997)8)
- 1.3 References
- Al-Sabbagh A et al. Antigen-driven peripheral immune tolerance: suppression of experimental autoimmune encephalomyelitis and collagen-induced arthritis by aerosol administration of myelin basic protein or type II collagen. Cellular Immunology, 1996; 171: 111-9
- Brandtzaeg P. History of oral tolerance and mucosal immunity. In: Weiner HW, Mayer LF (Eds.): Oral Tolerance: Mechanisms and Applications. Ann New York Acad Sci 1996; 778: 1-27
- Carvalho CR, Vaz NN. Indirect effects are independent of the way of tolerance induction. Scand Journal Immunology 1996; 6: 613-18
- Friedmann A, Weiner HL. Induction of energy or active suppression following oral tolerance is determined by antigen dosage. Proc Natl. Acad Sci USA 1994; 91: 6688-92
- Hahnemann S. Reine Arzneimittellehre. Dresden, 1811; ders.: Kleine med. Schriften, published by D. Ernst Stapf, Dresden and Leipzig, 1829; ders.: Unterricht für Wundärzte. Leipzig, 1789; ders.: Die chronischen Krankheiten. Dresden and Leipzig, 1835; ders.: Organon der Heilkunst. Dresden and Leipzig, 1829.
- Harisch H, Dittmann J. Untersuchungen zur Wirkung von Ubichinon Injeel and Injeel forte mit zellfreien Systemen. Biol Med 1997; 26(3):99-104
- Heine H. Lehrbuch der biologischen Medizin. 2. Auflage Stuttgart: Hippokrates 1997a
- Heine H. Neurogene Entzündung als Basis chronischer Schmerzen. Beziehun- gen zur antihomotoxischen Therapie. Vortrag 31. Med. Woche Baden-Baden, 01.11.97b (Biol. Medizin, in Druck)
- Reckeweg H-H. Homotoxikologie. Ganzheitsschau einer Synthese der Medizin. Baden-Baden: Aurelia, 1976
- Reckeweg H-H. Materia Medica Homoeopathia Anti-homotoxica. 3rd rev. English ed. Baden-Baden: Aurelia-Verlag, 1996.
- Weiner L, Mayer L. Oral Tolerance: Mechanisms and Applications. Ann New York Acad Sci 1996; 78: 1-418
- Weiner HL et al. Oral Tolerance: Immunologic mechanisms and treatment of animal and human organ specific autoimmune diseases by oral administration of autoantigens. Ann. Rev. Immunol. 1994; 12: 809-37
-
COLLAGEN MEDICAL DEVICE LUMBAR IN THE COMBINED TREATMENT OF LUMBAR INSTABILITYINDUCED PAIN
SUMMARY
Spondylolisthesis is a mechanical alteration in the physiological vertebral structure that is primarily characterised by the forward displacement of a part of or whole vertebra on to that below.
The L-S rachis segment is mostly interested.There are 3 kinds of Spondylolisthesis: dysplastic, due to osteo-articular congenital alterations; isthmic, characterized by a continuous lesion of the isthmus; degenerative.
- The aim of this study is to verify if a combined treatment, Physiokinesitherapy ultrasound-guided injection of Collagen MD (Medical Device)-Lumbar, may provide more important and durable clinical results rather than Physiokinesitherapy alone.
- 20 patients, F and M, aged between 40 and 75, have been enrolled; all of them suffering from grade 1 and 2 Spondylolisthesis.
They were randomised to 2 Groups (10 + 10 patients), a treated Group (T) and a control Group (NT).
The clinical results, evaluated at 2, 4, 8 and 12 months with the Numeric Rating Scale, the Oswestry Disability Index, the Pain Disability Index and the use of NSAIDs (number of tablets/week), allow to state that the combined treatment Physiokinesitherapy + MD-Lumbar obtains a far better and longer-lasting improvement than Physiokinesitherapy alone.
INTRODUCTION
Spondylolisthesis (SL) [from the Greek spóndilos (vertebra) and ólístesis (slipping)] is a mechanical alteration in the physiological vertebral structure that is primarily characterised by the forward displacement (anterolisthesis) of a part of or whole vertebra onto that below. Although SL can affect any segment of the spine, it is the lumbar segment that is most commonly affected. Various authors have estimated the incidence of SL in the general population to be 3-8%; however, it can affect up to 20% of the individuals involved in occupational activities or sports requiring hyperlordosis (e.g. artistic gymnastics, gymnastic rings, diving, golf) or in the handling of heavy loads (e.g. weightlifting).Clinicians are often called on to identify the origin of spinal pain and equally frequently forget that even a moderate spinal microinstability, such as SL, maybe the cause. One particularly important anatomical point in SL is the vertebral isthmus, the element between the superior and inferior apophyses that forms a connection between the anterior and posterior portion of the vertebra. Undoubtedly, one of the least resistant points of the spine is the lumbosacral junction (L5-S1), where the slope of the upper surface of S1 tends to cause the body of L1 to slip downwards and forwards. This displacement is restricted by the anatomical connections of the posterior arch of L5 and, in particular, by the isthmus.
SL occurs when the isthmus is subject to interruption or destruction. Furthermore, in addition to the osteoarticular structures, whose focal point are the spinal facet joints, seat to inflammatory processes developed over time driven by the pro-inflammatory cytokine network, the tendinous and ligamentous structures (e.g. the yellow ligament), the capsular structures, the intervertebral disc, the muscle structures (the multifidus muscle and the iliopsoas muscle) and the deep fasciae structures are also involved in the origin of SL-induced pain (mechanical low back pain).
• There are 3 main types of SL:
DYSPLASTIC
The dysplastic form is secondary to congenital osteocartilaginous alterations in the isthmus and consists of 2 main subtypes1) the form that is secondary to the sagittal orientation of the articular apophyses of S1 that lose contact with L5, which therefore slips forward;
2) the form that is secondary to the pathological elongation of the isthmuses of L5.
ISTHMIC
In most cases (80%), idiopathic bilateral isthmic lysis involves L5 and it is characterised by a fracture of the isthmus, which causes an increase in the size of the spinal canal, as the posterior portion remains in place
The inter-articular portion (i.e. isthmus) is the point of least resistance subject to continuous microtraumas that, together with other environmental and genetic factors, reduce its mechanical resilience.During development, isthmic SL often occurs following a minor trauma, thus revealing the underlying malformation. The signs and symptoms differ from those observed in adults; young patients experience mild pain without any specific topographical location, even in the presence of significant anterior displacement. In some cases, the only sign is hypertonia of the posterior thigh muscles, making it difficult to flex the limb at the hip with the knee extended.
DEGENERATIVE
The degenerative form is very common and is often little considered, partly due to the minimal likelihood of efficacious treatment, which constitutes the target of this study. Unlike isthmic SL, the degenerative form causes a reduction in the dimensions of the spinal canal; the favouring factors are the degeneration of the disc and of the articular apophyses, and an excessively vertical orientation of the articular apophyses.In addition to low back pain, it can also be associated with neurogenic claudication caused by spinal canal stenosis. Degenerative SL affects adults; it is caused by long-standing spinal instability and by alterations secondary to the abnormal displacement of the unstable segments, i.e. osteoarthritis and/or degenerative disc disease. This form is 4-6 times more common in females and affects L4 10 times more
frequently; the anterior displacement can be up as much as 33%.The degree of displacement is primarily assessed using the Meyerding Grading System, which classifies it into 4 grades: in grade 1, the displacement is equal to less than 25% of the upper surface of S1; in grade 2 it is less than 50%; in grade 3 it is less than 75%; in grade 4, the entity of the forward displacement can exceptionally reach 100%, with the potential displacement of L5 in the pelvis (Spondyloptosis). The intervertebral disc is inevitably involved; as it is no longer protected by the posterior structures, it absorbs functional overloads that exceed its anatomical characteristics, causing it to undergo a degenerative process that leads to flattening and, eventually, to herniation with an exacerbation of the pain symptoms of SL.

The nerve components are often involved with the compression of the dural sac and of the nerve roots of L5 and S1. The severity of the SL does not often correlate with the intensity of the pain symptoms.
The symptoms of SL are 1) mechanical low back pain, which is made worse by movement and improves with rest; 2) irradiation of pain to the lower limbs. Patients often experience a worsening of the pain when changing posture (from sitting to standing). The following symptoms are less common: discogenic low back pain that gets worse when seated and with the forward flexion of the upper body; facet joint pain that gets worse with the hyperextension of the upper body and when standing; neurogenic claudication
(lower extremity asthenia when walking) caused by the spinal canal stenosis that is often present.Anteroposterior, laterolateral and oblique projection x-rays, in addition to a dynamic x-ray study in the position of maximum anterior flexion and maximum extension, are essential for the diagnosis of SL. MRI is used to evaluate the possible compression of the nerve roots and any disc degeneration and/or bulging. It is not always simple to correlate instability (such as moderate degenerative SL) with pain symptoms and it is even more arduous to identify degenerative microinstability at an early stage. The real problem, however, is efficacious conservative treatment. Most patients with SL can be treated conservatively, especially in the presence of the grade 1 and 2 degenerative forms, in which the displacement evolves in approximately 50%of cases, depending on the case histories considered. The conservative treatment of SL is essentially physiotherapy-rehabilitationbased: the aim is not only to strengthen the muscles of the upper body in order to stabilize the spine, but also to improve the neuromotor and proprioceptive control of the pelvic girdle muscles, antigravity muscles and respiratory muscles. It is, of course, essential to re-educate the patient on how to maintain a good static and dynamic posture. In the acute phase, when the clinical situation is characterised by persistent low back pain, it is necessary to observe a suitable period of bed rest, associated with the administration of conventional and/or low-dose anti-inflammatories and muscle-relaxants, either individually or in combination. The optimisation of the conservative treatment of low back pain secondary to degenerative SL, taking into account all the anatomical structures involved in
this aetiopathogenesis, allows to formulate a number of considerations.COLLAGEN MEDICAL DEVICES
The use of injectable medical devices (MD) containing porcine collagen allows a more efficacious and specific in loco positioning of the collagen, with a carrier and stabilisation function. It makes it possible to replace, strengthen, structure and protect the cartilage, tendons, ligaments and joint capsules, thereby optimising the structure of the collagen fibres and of all the extra- and intra-articular structures in which it is present, thereby providing a mechanical support to the anatomical district in question.The hypothesis of the study was that a treatment with a specific injectable Collagen MD could re-condition the anatomical structure/s impaired by SL and improve the stability of the lumbosacral spine; that a “combined” treatment would have been able to improve the functional rehabilitation outcomes and/or provide more efficacious pain control in the subacute and chronic phases; and that a combined treatment would also have been able to positively condition the progression of SL with less frequent exacerbations.

MATERIALS AND METHODS
In order to explore this hypothesis, 20 patients with Physical Medicine outpatient clinic appointments for low back pain were recruited and included in the study, from January 2018 to January 2019. The patients were randomised to 2 treatment groups [T Group (Physiokinesis therapy + ultrasound-guided injections of MD-Lumbar) and the NT Group (Physiokinesis therapy alone)], stratified by age and gender; the outcomes were assessed at 2, 4, 8 and 12 months.Inclusion Criteria
F and M patients aged between 40 and 75 years; clinical and instrumental diagnosis of grade 1 and grade 2 Spondylolisthesis; NRS (Numeric Rating Scale) 5, no use of NSAIDs, corticosteroids or opioids.

Exclusion CriteriaRheumatoid arthritis, chondrocalcinosis, psoriasis, metabolic bone diseases, gout, active infections, clinical and instrumental diagnosis of grade 3 and grade 4 spondylolisthesis, spondylolysis, polyneuropathy, previous local/ epidural corticosteroid injections (> 3 years), use of oral corticosteroid and/or opioid therapy in the past 6 months, use of anticoagulants, pregnancy, mental diseases.
Both the T and the NT Groups were administered the same intra-hospital rehabilitation protocol (diagnostic and therapeutic care programme) based on neuromotor treatment for the proprioceptive reconditioning of the posterior back, lumbosacral girdle and respiratory muscles.The protocol also included ergonomic education and occupational therapy. The rehabilitation treatment consisted in: daily individual motor rehabilitation treatment for a total of ten 45-minute sessions; individual assessment by the occupational therapist at the 5th and 10th session; provision of a brochure illustrating the physiokinesis therapy exercises to be performed by patients at home and ergonomic advices; group treatment (max. 4 patients) one month after the last individual session, on 2 consecutive days, in 30-minute sessions.
• Group T (Treatment) also received ultrasound-guided injection therapy (Clarius Ultrasound portable system, Convex probe) according to the following protocol:
GUNA MD LUMBAR Pack of 10 Ampoules of 2ml – Urenus
5 sessions (1/week for 4 consecutive weeks and 1 after 15 days); 2 vials of MD-Lumbar per treatment. − Half a vial (1 mL) for each facet joint; 2 joints were treated at each treatment, alternating the upper and lower facet joints; at the 5th session the 2 most impaired joints (as shown by MRI) were treated.

A number of clinical and functional outcomes were investigated:
1) Numeric Rating Scale (NRS)
2) Oswestry Disability Index (ODI)
3) Pain Disability Index (PDI)
4) use of NSAIDs during the follow-up period (TABLES 1, 2 ,3 and 4).CONCLUSIONS
The data obtained (TAB. 5) allow to conclude that in the treatment of grade 1 and grade 2 Spondylolisthesis combined treatment with physiokinesis therapy + injection of MD-Lumbar makes it possible to obtain a far better and longerlasting improvement, in terms of- pain
- motor function
- impairment caused by spinal instability
- reduced use of NSAIDs.
Furthermore, the combined treatment proposed herein, for the first time in the treatment of Spondylolisthesis, would appear to allow a better control over disease progression and a reduction in exacerbations over time (pro-inflammatory cytokine network control).

From the data obtained, it emerges that:
− NRS. Group T (Physiokinesis therapy + ultrasound-guided injection therapy of MD-Lumbar) passes from 6.9 (T0) to 2.5 after 12 months (-63.8%).
Group NT (Physiokinesis therapy alone) passes from 7.1 (T0) to 5.7 after 12 months (-19.7%).
− ODI. Group T passes from 41.0 (T0) to 14.0 after 12 months (-65.9%). Group NT passes from 42.0 (T0) to 34.0 after 12 months (-19.1%).
− PDI. Group T passes from 64.0 (T0) to 38.0 after 12 months (-40.6%). Group NT passes from 62.0 (T0) to 64.0 after 12 months (±0%).
− NSAIDs (tablets/week). Group T passes from 1.3 at 2 months to 1.4 at 12 months (±0%). Group NT passes from 2.0 at 2 months to 3.0 at 12
months (+50%).MD-Lumbar improves the stability of the lumbosacral spine and organically reconditions the impaired anatomical structures (joint capsules, yellow ligament, antigravity muscles and connective deep fascia), thereby making a considerable contribution to the promotion of neuromotor and proprioceptive capacity.
Over the next few months, we hope to be able to confirm the results obtained by expanding the study sample and, in particular, to identify the optimum timing for further injection therapy with MD-Lumbar as part of an individual maintenance rehabilitation programme.
Literature
- Alfieri A., Gazzeri R. – The current managment
of lumbar spondylolisthesis. J. Neurosurg Sci.
57: 103; 2013. - Arvind G. et Al. – Should we label all synovial cysts
as unstable? Global Spine Journal. 7: 629; 2017. - Evans N. et Al. – Management of symptomatic
degenerative low-grade lumbar spondylolisthesis.
EFORT Open Rev. 3: 620; 2018. - Hildebrandt M. et Al. – Correlation between lumbar
dysfunction and fat infiltration in lumbar multifidus
muscles in patients with low back pain.
BMC musculoskeletal Disorders. 18: 12; 2017. - Huang K.Y. et Al. – The roles of IL 19 and IL 20 in
the infiammation of degenerative lumbar spondylolisthesis.
Journal of Inflammation. 15: 19; 2018. - Jae-Sung K. et Al. – Characterization of degenerative
human facet joints and facet joint capsular
tissues. Osteoarthritis Cartilage 23: 2242; 2015. - Massullo C. – I Guna Collagen Medical Device
nella ripresa funzionale dopo traumi sportivi.
La Med. Biol., 2017/2; 45-50. - Milani L. – Un nuovo e raffinato trattamento iniettivo
delle patologie algiche dell’Apparato locomotore.
Le proprietà bio-scaffold del collagene e
suo utilizzo clinico. La Med. Biol., 2010/3; 3-15. - Milani L. – I Guna Collagen Medical Devices 10
anni dopo. Analisi ragionata di 2 recenti importanti
ricerche e update della letteratura. La Med.
Biol., 2019/2; 3-18. - Pavelka K. et Al. – MD-Lumbar. MD-Muscle e
MD-Neural nella terapia locale del dolore lombare.
La Med. Biol., 2012/4; 13-17.
- Pavelka K. et Al. – Chronic Low Back Pain: Current
Pharmacotherapeutic Therapies and a New
Biological Approach. Current Medical Chemistry,
2018 May 13, 25: 1-8. - Russo G. – Portale Medicinafisica.it; 2019.
- Shahidi B. et Al. – Lumbar multifidus muscle degenerates
in individuals with chronic degenerative
lumbar spine pathology. J. Orthop Res. 35:
2700; 2017. - Tian G., Qi L. – Correlation between facet tropism
and lumbar degenerative disease: a retrospective
analysis. BMC Musculoskeletal Disorders, 18:
483; 2017. - Wagner S.C. et Al. – Severe lumbar disability is
associated with decreased psoas cross-sectional
area in degenerative spondylolistesis. Global
Spine Journal, 8: 716; 2018. - Zocco R. et Al. – Effectiveness of integrated
medicine in the control of pain in vertebral disorders:
observational study. Physiological Regulating
Medicine, 2012; 41.
Fig. p. 40
https://urbanministries.com/wp-content/uploads/2019/01/iStock-927091262-Pain.jpgFig. p. 41
Left:
https://eorthopod.com/images/ContentImages/spine/spine_lumbar/lumbar_spondylolistheis/lumbar_spondylolisthesis_cause02.jpg
Right:
https://www.brainspinesurgery.com/uploads/img/_800xAUTO_crop_center-center_60/Spondylolisthesis-Spine-Condition-and-Symptoms-Xrayy.png