DR. MED. W. THIEL
I. Introduction
One of the most important functions of the skin is to protect the organism against noxae and to guarantee regulated exchange of substances between the organism and its environment. If medicaments have to be brought into the organism by the percutaneous route, then this physiological protective barrier has to be overcome.
One method of transporting active substances through the skin into deeper lying tissue or to increase the extent of normal substance diffusion is direct current therapy. Transcutaneous ion transport, known as ionophoresis, is facilitated by this. Nevertheless, a prerequisite for this is that the pharmacologically active component of the dermatic is present in an electrically charged condition. According to whether the active substance is positively or negatively charged, the medicament is applied beneath the anode or cathode.
More recent studies⁴ ⁵ demonstrate that when ionophoresis is compared with diffusion, increased substance transport takes place only in the horny layer of the horrifying squamous cell layer. Since it is just this horny layer which represents the most effective barrier against diffusion of active substances, greater effectiveness can be achieved here by ionophoresis.
However, the active substances are spread within tissue layers lying below mainly by diffusion along the concentration gradient³.
With regard to the therapeutic effectiveness of this method, a pilot study³ after iontophoretic administration of a non-steroidal antirheumatic agent, humeral epicondylopathy being indicated, revealed a significant decrease in average pain intensity in the case of tenderness and total pain sensation, but further assessment features showed only a slight improvement. However, because of the lack of a comparative group, separation of the medicinal from the physical therapy effect was not possible.
In the case of ointments or gel preparations which contain only one medicament with positive or negative charge, substance transport of greater extent with the aid of direct current is evident because of conformity with natural physical laws¹. The therapeutic effectiveness of a combination treatment of direct current/medicament is also documented empirically elsewhere².
In the case of pharmaceutical mixtures, as are present in phytotherapeutic extracts and homeopathic preparations, it is not known as a rule whether the effective constituents are present in ionized form and if so, what charge they have. In addition there is the fact that it must be assumed in the case of these medicaments that several constituents which can also have different electrical charges are therapeutically effective.
The user can change the current direction at the iontophoresis unit in the course of therapy in order to be able to let both the positively and the negatively charged constituents through the skin into the tissue. Nevertheless, electrically neutral substances cannot be transported more quickly into foreign tissue by this method.
The objective of this investigation was to ascertain whether the combination of a Traumeel ointment therapy with iontophoresis has a better therapeutic result, i.e., faster restoration of health, than application of ointment alone. The therapeutic effectiveness of Traumeel ointment in distortions has been proven without doubt in the course of a double blind study⁶. Taking this effectiveness as proven, the therapeutic comparison of Traumeel ointment versus Traumeel ointment/direct current therapy was sufficient for us in this study without inclusion of a placebo.
II. Patients and methodology
A total of 50 patients with medium degree injuries were included in the study. All had the same type injury of external ligamentous overstretching in the sense of supination distortion trauma. 25 patients were treated exclusively with Traumeel ointment. The other 25 patients were subjected in addition to direct current therapy.
After the injury, immobilization in a Traumeel ointment dressing was provided for two days for all patients. No further dressings were applied after this.
One group of patients received following this a physiotherapy every 2 days in the shape of iontophoresis with a current intensity of 3 mA for a period of 10 minutes per session. The ointment was applied alternatingly for each patient both on the cathode and on the anode. Cold packs were applied in each case following this treatment. Traumeel ointment for daily self-application was prescribed to the patients of the other group. The patients were examined on the day of injury as well as on the 1st, 3rd, 5th, and 7th day. Assessment criteria were pain at rest, under pressure, and in motion, and were documented by means of a 4 point scale (0 = without, 1 = little, 2 = medium, 3 = severe). Furthermore, the circumference was measured with the aid of a tape measure over the narrowest point, the ankle, and the metatarsus. The mobility of the ankle joint was measured according to the neutral zero method. Circumference and mobility were compared with the healthy side in each case and the change in difference was evaluated. Since the patients were competitive athletes, the period up to the first day of return to athletic training was taken as the criterion for assessing the therapy.
III. Results
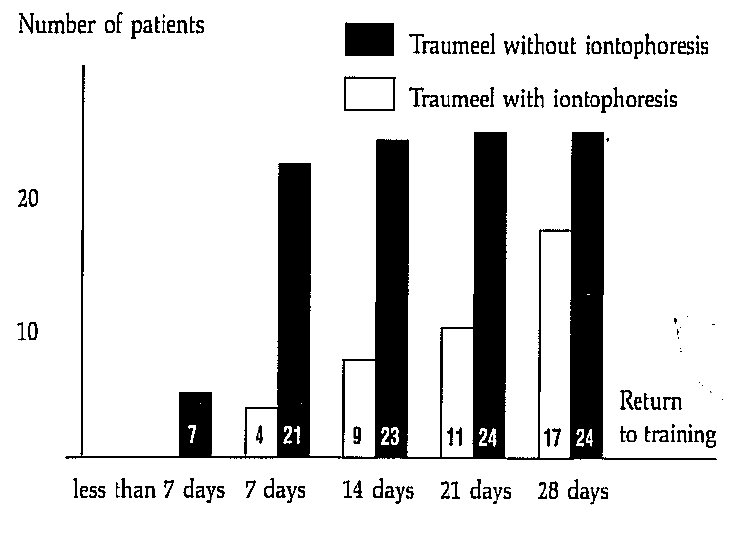
1. Return to training
If the two groups are compared with one another with regard to the first day of return to training, it results that more patients in the group treated solely with Traumeel ointment returned to training at an earlier point in time.
Fig. 1: Return to Training
2. Pain at rest
Fig. 2: Course of the average pain at rest values
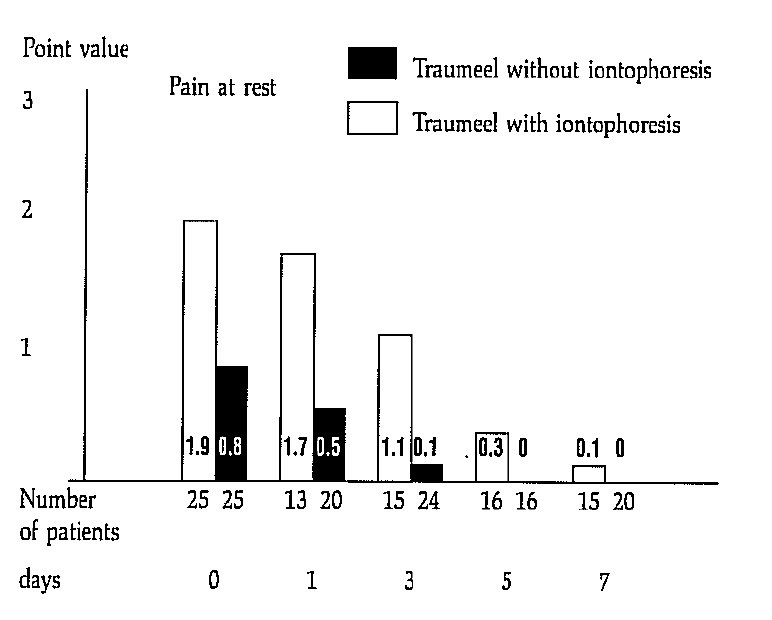
The intensity of the pain at rest was documented in the shape of point values on the 1st, 3rd, 5th, and 7th day of treatment.
The starting value of the two groups were different (with iontophoresis 1.9; without iontophoresis 0.8), so that a comparison of the course with regard to this feature could be made only conditionally. However, it can easily be seen from Figure 2 that both starting values decreased over the 7 days continuously and in a comparable ratio. In the group treated only with ointment, the value of 0.1 was reached for pain at rest within 3 days because of the low starting value; in the iontophoresis group, this value was reached only on the 7th day. (However, the higher starting values existed here.)
Since various patients did not appear at some appointments for “nonmedical reasons”, the starting values of these dropping out patients were analyzed separately. Since these were not extreme values, the average trend values of the assessment features were not distorted by the lack of these data.
3. Pain on pressure
Fig. 3: Course of the average pain on pressure values
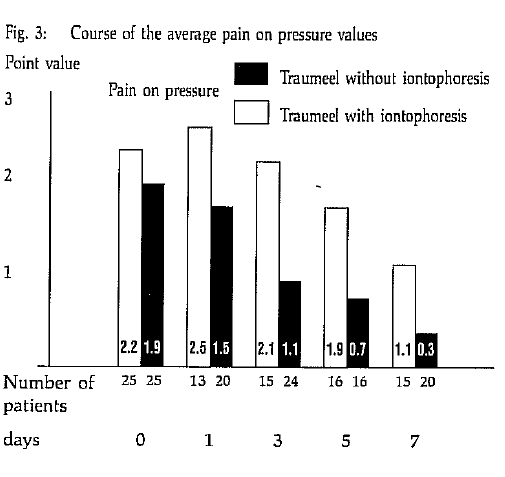
The starting values in both groups were comparable with regard to this feature (iontophoresis group on average 2.2; Traumeel group on average 1.9). The intensity of pain on pressure also decreased here continuously as can be seen in Figure 3 from 1.9 points to 0.3 points. In the iontophoresis group, the average pain intensity increased at the beginning (from 2.2 to 2.5) and then decreased continuously but significantly slower than in the Traumeel group. On the 7th day of observation, an average residual pain on pressure of 1.1 was still present.
4. Pain on movement
Fig. 4: Course of the average pain on movement values
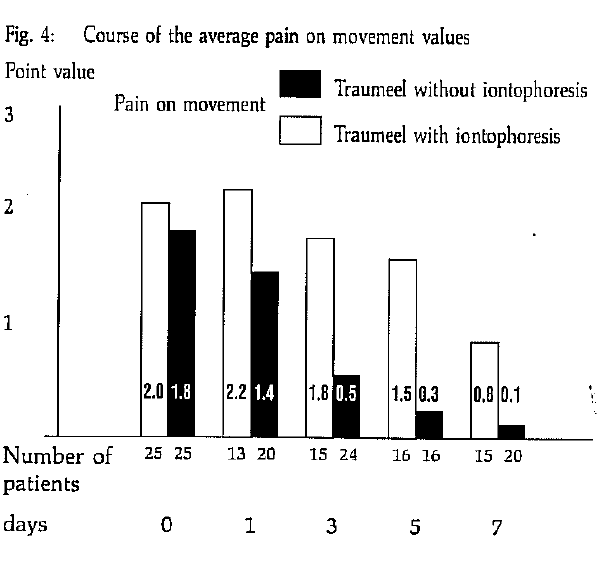
The starting values of both groups were also comparable in the case of this feature (iontophoresis group on average 2.2; Traumeel group on average 1.9). The intensity of pain on movement also decreased here continuously as can be seen in Figure 4 from 2.0 points to 0.3 points.
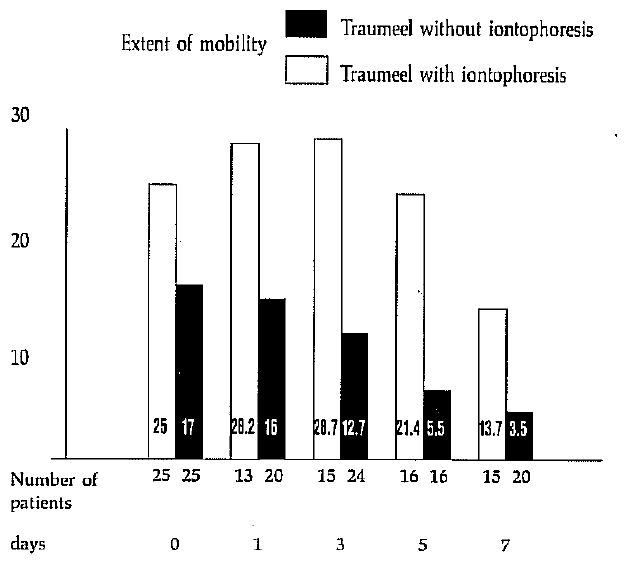
5. Mobility
The mobility of the healthy and injured joint was measured according to the neutral zero method and the difference between the two values was formed.
In the Traumeel group, this difference decreased to the value of 3.8° on the 7th day, a negligible value, which lies in the range of the error limits. In the iontophoresis group, a residual angle difference of 10.7° remained on the 7th day after initial deterioration (Fig. 5).
Fig. 5: Course of the average extent of mobility
(Difference between injured and healthy joint)
6. Circumferential measurements
The data of the circumferential measurements are only conditionally suitable for interpretation (see discussion), since the spread (see table 1) and the value range are too large.
IV. Discussion
In orthopedic traumatology, there is a trend towards treating the consequences of injury with antiphlogistic ointments and to make therapeutic use of the stimulating effect of direct current treatment (galvanization). The ionization of the active substance is considered to be secondary.
As can be seen from the above tables, an increase in swelling in the ankle joint region was noticed in the control examinations in the iontophoresis group. This is attributable to a condition of irritation caused by electrotherapy as well as to sacculation of the hematoma of the distal joints of the metatarsus.
On critical comparison of the two forms of application of iontophoresis and simple treatment with ointments after inital elastotape dressing, the latter musgt be given preference because of the more rapid incidence of effect, in particular for competitive athletes. Exclusive ointment application has also the advantage of being free of irritation. Side effects were not observed in any patient.
On the other hand, iontophoresis has proven itself for patients who cannot tolerate adhesive dressings for several days (lacing effect in varicosis) or who themselves cannot rub in ointments for certain reasons (older people, disabled etc.). Application of ointment alone, i.e. without initial tape dressings, should be performed only for simple bagatelle injuries which require no specific medical supervision.
Literature
- Pratzel, H., Die Iontophorese, Med.-Info Nr. 1 (Transcutan GmbH)
- Magyarosy, J., Ernst, E., Marr, N., Schmolzl, Ch., …
- Schops, P., Seichert, N., Erdl, R., Siebert, W., Pratzel, H., Pilotstudie zur klinischen Wirksamkeit einer definierten Iontophorese mit Indometacin bei Epicondylopathia humeria, Z. Phys. Med. Baln. Klin. 15, 395–399 (1986)
- Pratzel, H., Grundlagen des perkutanen Stofftransports in der Pharmako-Physio-Therapie und Balneotherapie, Dissertation 1985 (quoted in 3)
- Pratzel, H., Machens, R., Dittrich, P., Iontophorese zur forcierten Hautresorption von Indometacin und Salicylsaure, Z. Rheumatol. 104, 40, 748 (1986) (quoted in 3)
- Zell, et al., publication in preparation
Address of the author:
Dr. med. Werner Thiel
Orthopedic physician
Kirchstraße 9
D‑6635 Bous
Germany