There are very few patients who don’t need detoxification and drainage intervention at all. Furthermore, each patient’s status is unique, so in designing a treatment plan, it is important to strike a balance between the patient’s previous exposure (toxic load) and the organism’s ability to detoxify (regulation ability).
For this purpose, patients are generally divided into two groups. Group 1 includes patients with mild to moderate toxicity. In general, these are patients with mild symptoms and exposure. They elect to do a general cleansing or have milder diseases such as headaches, acne, etc. Group 2 includes patients with severe toxicity (known exposure) as well as patients with severe diseases such as cancer, autoimmune diseases, etc. These patients’ regulation ability is reduced. Group 2 also includes former drug addicts as well as patients who have received chemotherapy.
Due to their advanced toxicity, Group 2 patients need advanced supportive detoxification that prepares the organs of detoxification and elimination for the drainage phase (accomplished primarily through Lymphomyosot, a component of the Detox-Kit). The advanced organ support is thus more organotropic in character, whereas the basic detoxification and drainage is more functiotropic. In general, advanced organ support is administered for six weeks, followed by use of the Detox-Kit. In most cases, tissues will still need to be drained of residual toxins, so the use of Lymphomyosot alone is advised for several months longer (for protocols, see BT Winter 2007).
Special case 1:
Patients with inflammatory skin disease, such as eczema or psoriasis. The skin, classically called the “mirror of the soul,” is also a mirror of the liver and the gut. In cases of skin disease, it is essential to remember that the P450-containing system in the skin is the same as that in the liver and in the gut. Psoriasis patients in particular need bowel cleansing, which should be part of the initial advanced organ support. Thus Mucosa compositum and Cutis Compositum play a special role in these patients, although functiotropic medications such as Nux vomica-Homaccord, Berberis-Homaccord, and Lymphomyosot, along with Hepeel, are the mainstays in the treatment of skin disease. Patients with inflammatory skin disease are at high risk of flare-ups if toxin drainage is initiated before the liver and gut are ready to cope with the load. These patients need to be treated with care even though they may not seem very ill. In some cases, flare-ups will simply mean that patients need higher doses of cortisone, but in other cases hospitalization may become necessary if skin sloughing is severe.
Patients with eczema are in a Th2 rigidity state, so they should first undergo several weeks of initial immunomodulation to get the disease under control, followed by advanced organ support, before the drainage period is initiated. Engystol is the medication of choice together with the appropriate suis-organ preparation, in this case Cutis compositum. By contrast, patients with psoriasis are in a Th1 state, so they should be treated with Traumeel oral ampoules and Cutis compositum. In both cases, it is preferable to add the catalysts during the drainage phase rather than during advanced organ support (see protocol in Table 1).
Table 1: Protocol for inflammatory skin disease
Disease-Specific Treatment
For Th1 rigidity: Traumeel and Cutis compositum For Th2 rigidity: Engystol and Cutis compositum Schwef-Heel
Weeks 1–4(or even longer in severe cases)
Organ/System
Treatment
Liver
—
Urinary tract/Kidney
—
Lymph
—
Skin
Cutis compositum
Gut
Mucosa compositum
Connective tissue
—
Note: Due to the high incidence of leaky gut in inflammatory skin diseases, initial treatment of the gut and immune system is paramount. The suis organs induce Th3 cells and thus immunotolerance to the corresponding organs.
Dosage:
Ampoules: In general, 3–1 times weekly, 1 ampoule i.m., s.c., i.d.
Drops: In general, 10 drops 3 times daily
Advanced Organ Support
Duration: 6 weeks
Organ/System
Primary Treatment
Alternative Products
Liver
Hepar compositum
Hepeel
Urinary tract/Kidney
Solidago compositum
Reneel
Lymph
—
Galium-Heel / Lymphomyosot
Skin
Cutis compositum
Schwef-Heel
Gut
Mucosa compositum
Nux vomica-Homaccord
Connective tissue
Thyreoidea compositum
Pulsatilla compositum
Basic Detoxification and Drainage
Organ/System
Detox Treatment
Cellular Detox (Add)
Liver
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Urinary tract/Kidney
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Lymph
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Skin
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Gut
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Connective tissue
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Note: Because Schwef-Heel is a potency chord, it does not cause aggravation to the extent classically ascribed to sulfur-containing medications. Adjuvant use of probiotics throughout the treatment should be considered.
Dosage:
Ampoules: In general, 3–1 times weekly, 1 ampoule i.m., s.c., i.d.
Drops: In general, 10 drops 3 times daily
Practical Protocols
Chronic fatigue syndrome is a complex and highly debilitating disorder characterized by chronic mental and physical exhaustion. It occurs more often, but not exclusively, in women.
Special case 2: Patients with chronic fatigue syndrome.
All patients with chronic fatigue syndrome have some form of toxicity. Some of these patients present primarily with symptoms of intoxication and have a history of toxic exposure, often temporally related to the onset of the syndrome.
Due to general immune imbalance (Th2 rigidity) and mitochondrial impairment in these patients, advanced organ support is essential, but even before that, support for the mucous membranes, the immune system, and the neuroendocrine system is helpful. This is best done with a combination of Mucosa compositum and Tonsilla compositum. After two weeks, advanced organ support can begin, followed by the drainage phase. If relapse occurs during the drainage phase, advanced organ support should be resumed for at least another six weeks (see protocol in Table 2).
Table 2: Protocol for chronic fatigue syndrome
Disease-Specific Treatment: Aletris-Heel
Followed by detoxification therapy
Weeks 1–2
Organ/System
Treatment
Liver
—
Urinary tract/Kidney
—
Lymph
Tonsilla compositum
Gut
Mucosa compositum
Connective tissue
—
Weeks 3–8: Advanced Organ Support
Organ/System
Primary Treatment
Alternative Products
Liver
Hepar compositum
Hepeel
Urinary tract/Kidney
Solidago compositum
Reneel
Lymph
Tonsilla compositum
Galium-Heel
Gut
Mucosa compositum
Nux vomica-Homaccord
Connective tissue
Thyreoidea compositum
Pulsatilla compositum
Weeks 9–20: Basic Detoxification and Drainage
Organ/System
Detox Treatment
Cellular Detox (Add)
Liver
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Urinary tract/Kidney
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Lymph
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Gut
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Connective tissue
Detox-Kit
Coenzyme compositum / Ubichinon compositum
Note: These patients need very gradual treatment. Because they often have multiple chemical sensitivities, it is advisable to first restore the integrity of the gut lining while administering Tonsilla compositum to support the adrenals and the hypothalamus. This also supports the immune system.
Dosage:
Ampoules: In general, 3–1 times weekly, 1 ampoule i.m., s.c., i.d.
The dental profession is becoming increasingly aware of the indivisibility of dental health and overall health. The teeth, the tongue, the gingiva, the lips, the salivary glands, etc. are all integrated with the rest of the body via the nerves, the blood and lymphatic circulations, glandular secretions, acupuncture meridians, the connecting bones and joints and by the digestive tube which extends from the mouth to the anus.
Because of the mechanical nature of most dental therapeutic procedures it may occasionally be convenient to forget that the mouth we are treating is connected to a vital, breathing, thinking, feeling human being. Yet the profound interrelationships between the mouth and the rest of the body have been recognized in the scientific literature of the West for several decades and by the Chinese for some fifty centuries.
When treating someone with an oral health problem, often the cause is found locally—such as a broken tooth due to trauma, a lost filling, or a sore spot from an ill-fitting denture. But more frequently the cause is found outside the mouth. This is particularly true of the more chronic oral maladies, such as periodontal disease, temporomandibular joint (TMJ) disorders, oral cancers, bruxism, bad breath, herpes simplex, tooth decay and, more recently, AIDS. Other common examples of this remote causation of oral pathology include the severe alveolar bone resorption found around the roots of the teeth in the diabetic patient,⁴ and the gross proliferation of fibrous tissue of the gingiva in the epileptic patient receiving Dilantin therapy.⁵ Even the American Dental Association now recognizes this systemic causation of periodontal disease.³ The dentist is sought out for evaluation and treatment of these oral symptoms—despite the fact that these oral symptoms are merely a localized manifestation of a more systemic disturbance.
Perhaps less widely appreciated but, I maintain, more frequent in occurrence are those systemic maladies which result from oral sources—as has been elaborately described and documented by Dr. Rheinhold Voll,⁴ and others.⁵ ⁶ Typical examples include the constipation of the TMJ patient due to his impaired chewing ability, or the migraine headaches of a mercury-hypersensitive physician provoked by a mouthful of amalgam (50% Hg) fillings, or the abdominal rash of the nickel-hypersensitive woman elicited by placing a nickel crown on her tooth. In these cases, ironically, the patients traditionally must seek the treatment of a physician (rather than the dentist) because of the systemic nature of the symptoms—despite their oral origins.
Consider that only a few decades ago it was fairly common “medical” treatment for rheumatoid arthritis to extract all the patient’s teeth—frequently with great success. One cannot soberly ignore the fact that what we do in our dental treatment can profoundly affect that individual’s systemic health and vice versa.
Once this concept is embraced, then the role of homeopathy in dentistry is much easier to appreciate. We will look at both acute and chronic dental prescribing, in this paper, and then explore the three basic constitutional types.
ACUTE DENTAL PRESCRIBING
Over the years I have found that a handful of remedies can handle the majority of the acute dental emergencies with which I have been faced in my practice. These first-aid remedies can help alleviate the pain or discomfort of dental emergencies, at least temporarily, until proper dental care measures can be received. I must emphasize, however, that the remedial measures proposed herein are not intended to replace good dental care, but rather to serve as a safe and effective complement to good dental care. (The potencies mentioned below are only suggestions. These are the ones I have used in my practice. A 30C should work as well as a 30X. As in all homeopathic prescribing, the remedy selection is more important than the potency. In other words, if the case calls for Belladonna 30X and all you have is Belladonna 6C, use it!)
Abscesses
Belladonna. Early dental abscesses, accompanied by redness and throbbing which is aggravated by the slightest touch (30X every 30–60 minutes).
Hepar sulphuris calcareum. Where the abscess is accompanied by pus formation, increased salivation, and where the gums are sore to the touch and bleed easily. Repeated doses of 6X will encourage pus discharge, while higher potencies (30X–200, two or three times daily) will help abort pus formation.
Silicea. Once pus is draining, Silicea 6X a few times daily will hasten the discharge.
Myristica. Where the abscess is swollen and accompanied by numbness of the area. Especially suited to the wisdom teeth. (6X)
Calendula. Dilute the tincture 1 part to 20 parts of water. Use as a gentle but effective disinfectant mouth rinse. This may be used several times daily (with any of the above remedies or by itself) or may be alternated with warm salt water rinses.
Apprehension (anticipation of the dental visit)
Gelsemium. Fear accompanied by “weak knees,” diarrhea, and drowsy behavior. 30X to be taken the night before, the morning of and ½ to 1 hour before the dental visit.
Aconite. When the fear is accompanied by great panic (sudden onset) as well as physical and emotional restlessness (e.g., much fidgeting). 30X taken as above.
Coffea cruda. 30X is helpful when the anxiety is accompanied by intolerance to noise or music.
Chamomilla. This is not for apprehension, per se, but may greatly help those individuals with lowered pain thresholds. Take three doses of 30X over several hours prior to the dental visit.
Bleeding
Almost all post-surgical bleeding is well controlled by pressing a moist gauze pad or moist tea bag over the bleeding area. However, when this alone does not control the bleeding:
Phosphorus. 6X to 200X every 10 to 30 minutes until the bleeding stops.
Arnica. If bleeding is accompanied by bruised soreness. 30X every 10 to 30 minutes until bleeding is controlled.
“Dry Socket”
Belladonna. 30X every 30 to 60 minutes if accompanied by a throbbing pain.
Ruta graveolens. 6X for any surgery or other injuries to the jaw or other facial bones.
Calendula. As prepared above is a good healing rinse.
Teething
Chamomilla 30X every 30–60 minutes when the teething child is whiney, restless, and wants to be held and pampered. This is a great remedy for delayed and difficult teething.
Toothaches
Belladonna. 30X every 30 to 60 minutes when the toothache throbs and is worse from touch or motion (chewing).
Magnesia phosphorica. 30X when the toothache is worse from cold and better from warmth.
Coffea cruda. 30X when the toothache is worse from heat and relieved by holding ice in the mouth.
Chamomilla. 30X when the toothache is worse from any warmth (i.e. if anything warm is taken in the mouth or even upon entering a warm room), but not better with cold. The pain is intolerable and makes the patient peevish.
Dental Trauma (or Post Operative) Remedies
Arnica. 30X for injuries resulting in bruises or fractures; for sore spots from an ill-fitting denture; following the placement of a very deep filling. (Many patients find Arnica helpful when taken before a dental visit where discomfort is anticipated)
Hypericum. 30X where nerves have been injured—such as a broken tooth where the nerve has been exposed, and accompanied by excessive pain.
Ledum. 30X for puncture wounds, such as the soreness resulting from a dental injection.
Staphysagria. 30X for incision type wounds after soft tissue surgery—as with extractions of difficult impacted wisdom teeth or periodontal (gum) surgery.
Chamomilla. Helps expedite the wearing off of the numbness following the completion of the dental procedure. 30X every 20 to 30 minutes. Works beautifully!
Magnesia phosphorica. 30X for stiff, sore jaws following a prolonged dental visit with the mouth wide open where the muscles are cramped and feel better with warmth. If they don’t feel better with warmth, try Arnica 30X instead.
CHRONIC DENTAL PRESCRIBING
Now that we have looked at some of the homeopathic treatments for a few of the more common acute dental problems, I would like to explore the role of homeopathy in the treatment of chronic dental or oro-facial complaints. To evaluate and treat someone for a chronic dental problem (i.e. periodontal disease, chronic TMJ disorders, bruxism, or rampant tooth decay) one must exercise the same deliberation as when treating any other chronic conditions—that is, a thorough history and examination must be done. To give adequate scope to the ongoing disease process and its various causes, one must include not only the dental manifestations, but all levels of the patient’s symptoms (physical, mental, emotional, and spiritual) in the evaluation. “How can a dentist evaluate one’s mental condition?” you ask. Remember, the repertories and materia medicas are written (gratefully) in plain English—not in “medicalese.” One needn’t be skilled in abnormal psychology to see that a patient is frightened, cheerful, or angry. One need only observe and listen!
Dentists have particular expertise in evaluating a person’s oro-facial signs and symptoms (which, incidentally, comprise a very significant portion of Kent’s Repertory), and this is the focus of our therapy. However we are sometimes criticized for “practicing medicine without a license” because through appropriate “dental” therapy the patient’s “medical” condition improves. The reader will understand from the initial discussion in this paper the error of such thinking. Furthermore, homeopathic remedies (like allopathic drugs) are not organ specific. They affect the entire person. Thus, when you visit a dentist complaining of a swollen jaw and he gives penicillin for the infected wisdom tooth, doesn’t your infected hangnail respond to the medicine as well? Likewise, even though it may not be our intention to witness a cure of sciatica or dyspepsia with correct dental treatment, such things do happen and, as with the infected hangnail, this obviously does not imply that we are practicing medicine. Remember, it is the individual’s vital force, not the prescriber’s intentions, that directs the evolution of cure, as the case below well illustrates.
Over the past twelve years a large portion of my practice has dealt with the care and treatment of people suffering from disorders of the temporomandibular joint (TM joint or jaw joint). This paired joint connects the lower jaw to the skull and lies just in front of the ears. Because disorders of this joint cause such profound and diverse sequelae in the patient’s overall health, they serve as a good vehicle to illustrate the indivisibility of oral and systemic health. The various signs and symptoms of TM joint disorders fully permeate one fourth of the pages of Kent’s Repertory. They include headache, earaches, grinding and popping noises in the joint, vertigo, pains in the neck, shoulders, and back, indigestion, poor balance, unstable posture, and many others.
CASE HISTORY
On July 25, 1983 a 20-year-old woman presented with a constant headache which had begun 12 months before. The headache was worse upon awakening in the morning and began one month after leaving home to attend college. She had difficulty eating because chewing caused pains in the right temple. She also suffered from chronic constipation, insomnia, and fatigue. She appeared pale, unsmiling, and listless and she had not had her menses for seven months. Prior treatments had been of little help and included therapy by neurologists, gynecologists, a psychiatrist, an allergist, internist, nutritionists, acupuncturist, chiropractors, dentists, a cranial osteopath, and a neurolinguistic programmer. She had a history of other head injuries. She was given Arnica in high attenuation.
Two months later she reported no significant change in her health. She was fitted with an orthopedic appliance and put on an exercise program to help alleviate her jaw muscle tension. Within days she began to sleep better, but over the next few months the headaches were still constant, although diminished. She still had no menses, was thirstless and still constipated. She was given Natrum muriaticum 1M.
Natrum muriaticum has headaches, worse in the morning as part of the remedy picture. Also included are a great variety of menstrual complaints, constipation, difficulty sleeping, and emaciation. It is the chronic of Ignatia, often, as Boericke says, “having psychic causes of disease”* (i.e. leaving home).
When she returned a month later, her appearance had dramatically improved. Her face was more animated, her dress more colorful, and her voice more vibrant. She was sleeping well and her head and jaw pains had markedly lessened. Her cranial osteopath reported the first profound improvement in her cranial mechanism since he had begun treating her. Several days after the remedy was given she had her first menses in almost a year.
THREE CONSTITUTIONAL TYPES
In taking a case of a chronic dental patient one can garner a great deal of information as to the patient’s constitutional type by examining his or her oral and cranial structures. Here I must define “constitutional” in its narrowest sense, based on the theory of constitutional typing by Nebel and Vannier, also referred to by Professor Eizayaga, M.D., as the “genotypical” constitutional type. That is, the constitution is the least changeable aspect of the person’s totality; it is based largely on the structure and composition of one’s tissues and skeletal framework, and therefore is immutable and established long before birth.
Our skeletal and dental structures are composed of three calcium salts (or Calcareas): the carbonate, phosphate, and fluoride. Each of these salts impregnates our teeth and bones and thereby imparts to us distinctly different anatomical characteristics, different metabolic types, as well as different disease propensities. Accordingly, everyone belongs to one of these three constitutional types: Calcarea carbonica, Calcarea phosphorica, or Calcarea fluorica, depending upon which salt predominates in our makeup. Furthermore, to each of these constitutional types belong a group of remedies or “phenotypical” constitutional types (Eizayaga). While it is common to see individuals who exhibit combinations of these three constitutional types (especially mixtures of the phosphor-fluor and fluoric-mixed type), one type will always predominate.
As we shall see, nowhere are the anatomical differences among the Calcareas more dramatically illustrated than in the dental apparatus. Thus the dentist has a unique vantage for assessing a patient’s constitutional type, and therefore can gain much insight into that individual’s therapeutical needs. The information I am presenting here is largely lacking in the homeopathic Materia Medicas and I am therefore greatly indebted to M. Tetau, M.D., F. Fuller Royal, M.D., and E. Illovici, M.D., for their writings which helped consolidate the constitutional pictures you are about to meet.
Calcarea Carbonica
The carbonica has broad shoulders, a broad forehead and large jaws. The teeth are very white and well aligned but are slow to erupt with difficult teething. The fontanelles of his very large skull are slow to close and his head perspires easily. His tongue is dry, he does not like to talk, and his teeth cannot endure any coldness—even cold air!
The carbonica resembles the oyster shell from which the remedy is made, that is, he is resistant to change—“a victim of inertia.” Yet, while slow to begin a project, he will, once started, continually plod ahead until the job is completed. While not terribly imaginative, he is logical and is good with mathematics (many mathematicians and accountants are carbonicas).
His long bones and spine are curved, and his bones, joints, and muscles are as rigid and inflexible as his opinions. He tends to develop hypertension, hypothyroidism, obesity, and autointoxication due to his failure to remove toxins adequately from his body. The child exhibits delayed puberty and is frequently troubled by bedwetting. He is chubby, his complexion has a chalky tint, and he is prone to digestive complaints.
Major remedies related to the Calcarea Carbonica type aid in the elimination of the body’s toxins: Sulphur, Hepar sulph., Graphites, Silicea, Carb. veg., and Lycopodium.
Calcarea Phosphorica
The phosphoricum type is mentally precocious and develops early. He is tall with long arms and legs and his back is stooped. The skull is long (front to back) and narrow, as are the jaws. The forehead is elevated and the nose strong. The teeth are oval and have a yellow cast to them. The palate is narrow with a gothic (high) vault.
He is very imaginative and artistic and does not tolerate manual labor or any regularity in his life style. Because he cannot stay with any task for very long, he seldom masters anything—despite being a perfectionist at heart.
He has long eyelashes, his hair is fine, and his skin delicate. When he perspires, he does so all over. He tends toward hyperthyroidism, palpitations, and tuberculosis.
Major remedies related to the phosphoricum constitutional type are Natrum mur., Ferrum, Kali carb., Iodium, Arsenicum album, Phosphorus, and Stannum.
Calcarea Fluoricum
The fluoricum constitution is the picture of instability both mentally and physically. The bones are deformed and the muscles and ligaments are very lax, producing an “S”-shaped posture. The arms hyperextend at the elbows. The dental arch and alignment of the teeth are irregular. The upper jaw protrudes, the feet are abnormally small and the hair is hard and brittle.
He dislikes exercise and has little physical endurance. He cannot concentrate on anything for long periods of time and seldom perspires at all. His temperament is unstable, he has little control over his reactions, and will say whatever is on his mind. All of his symptoms are worse at night but he feels better in the mountains. He tends toward arteriosclerosis, arthritis, and hypertension.
The major remedies that relate to the fluoricum constitutional type are: Mercurius, Aurum metallicum, Argentum nitricum, Kali bichromicum, Platina, Nitricum acidum, Baryta carbonica, and Syphilinum.
The following chart summarizes the characteristics of the three calcareas groups:
ANATOMICAL AND ORO-FACIAL KEYNOTES (including TMJ)
Keynote
Calcarea carbonica
Calcarea phosphorica
Calcarea fluorica
Skeleton
Resistant
Fragile
Irregular, exostoses
Hand
Strong & thick
Long & narrow
Small, soft & pliable
Perspiration
Localized to head & neck
All over
Very little (skin dry)
Athletic type
Good endurance (fullback)
Lacks endurance but has brilliant bursts of energy (quarterback)
Not well coordinated (team mascot)
Oro-facial
Large, broad head, open fontanelles
Elongated head, open fontanelles
Asymmetrical head
Jaws & Arches
Large elliptical
Narrow elongated elliptical
V-shaped, irregular
Vault (Palate)
Low
Gothic
Narrow & very deep
Tooth Eruption
Delayed & difficult dentition
Early but painful teething
Teeth erupt out of normal sequence
Teeth
White with broad stocky crowns. Upper incisors flat & square. Sensitive to cold
Yellow & long. Upper incisors rectangular with curved facial surfaces
Grey-white teeth. Gum boils, sensitive to pressure & eating, looseness of teeth
Occlusion (bite)
Teeth well aligned
Often malposition in anterior teeth
Irregularly set into arches with sagittal (forward or backward) malposition
TM Joint
Strong & tight
Fine & slack
Hyper-stretch
CONCLUSION
This paper presents a brief overview of the role of homeopathy in dentistry as it relates to acute and chronic prescribing and to the three basic constitutional types. Correct homeopathic prescribing for dental maladies will frequently provoke salutary systemic effects, and this should neither threaten nor alarm us. This is simply a reflection of the natural law of cure and illustrates the fact that the dental apparatus is an indivisible component of the integrated whole person. It cannot be otherwise! And for this we should all be grateful—doctor and patient alike.
“Etiology of Chronic Periodontal Disease: An Alternative Perspective,” Clark & Carey, Journal of the American Dental Association, Vol 110, May, 1985, pp. 583–589.
Interrelation of Odontons and Tissues in Organs, Field Disturbances and Tissue System, Rheinhold Voll, M.D., M.L. Publishers, Dijal Velzen, West Germany, 1976.
Neural Focal Dentistry—Illness Caused by Interference Fields in the Trigeminal, Ernesto Adler, M.D., D.D.S., Multidiscipline Research Foundation, Houston, 1984.
Electric Acupuncture for Dentistry, John Chan, D.D.S., Nutri-Kinetic Dynamics, Inc., Pearl City, Hawaii, 1980.
Repertory of the Homeopathic Materia Medica, J.T. Kent, A.M., M.D., Indian Books & Periodicals Syndicate, Box 2524, Karol Bagh, New Delhi, 110005.
Materia Medica with Repertory, 6th ed., William Boericke, M.D., B. Jain Publishers, New Delhi, 110055.
“Homeopathy, Holistic Medicine: Terrain, Constitution, Temperament.” M. Tetau, M.D., Journal of Ultra Molecular Medicine, Vol. 1, No. 3, Las Vegas, NV, 1983.
“Understanding Homeopathic Constitutions, Part I.” F. Fuller Royal, M.D., Journal of Ultra Molecular Medicine, Vol. 1, No. 2, Las Vegas, NV, 1983.
“Understanding Homeopathic Constitutions,” Part II. F. Fuller Royal, M.D., Journal of Ultra Molecular Medicine, Vol. 1, No. 3, Las Vegas, NV, 1983.
“A New Concept in Essential Homeopathic Mineral Compositions.” Emile Illovici, M.D., Journal of Ultra Molecular Medicine, Vol. 1, No. 3, Las Vegas, NV, 1983.
“Homeopathy with a Dental Accent.” Richard D. Fischer, D.D.S., F.A.C.D., Homeopathy Today, National Center for Homeopathy, Washington, D.C., March, 1984.
Personal Communication, Kathrine Coulter.
Recommended Reading
A New Approach to Oral and Dental Disease, Frank W. Stockton, D.D.S., National Center for Homeopathy, Washington, DC. The Dental Prescriber, Dr. Colin Lessell. The British Homeopathic Association, 27a Devonshire Street, London.
ESTIMATION OF CLINIC AND IMMUNOLOGIC EFFECTIVENESS OF THE USING OF PSORINOHEEL, LYMPHOMYOSOT AND MUCOSA COMPOSITUM S IN COMPLEX TREATMENT OF ATOPIC DERMATITIS IN CHILDREN
Rudenko I.V. Lugansk State Medical University
Summary Investigation of genetic background, cell immunity, condition of hepatobiliary system, biocenosis of intestine and important allergens in children suffering from atopic dermatitis was conducted.
82 children were examined. The control group included 39 children with age ranging from 3 to 14 years. The main group included 43 children. In the main group patients received complex therapy with antihomotoxic preparations in age dosages.
Psorinoheel – from 2 to 10 drops 3 times a day during 3 months.
Lymphomyosot – from 2 to 20 drops 3 times a day during 3 months.
Mucosa compositum S – from 1/6 to 1 ampoule i/m 3 times a week during 2 weeks with further injection once a week during 3-4 weeks.
The treatment was prescribed for all patients in the stage of exacerbation.
Data of cell immunity were investigated before and after the treatment.
In the main group reliable improvement of functional activity of lymphocytes, decreasing their suppressive activity, normalizing of immune index was noted.
Intestine bacterial flora was normalized, positive influence on hepatobiliary system and stable clinic remission was noted.
Received results allow recommending antihomotoxic therapy with combination of preparations Psorinoheel, Lymphomyosot and Mucosa compositum S in children suffering from atopic dermatitis.
COMPLEX TREATMENT OF PATIENTS SUFFERING FROM DISCIRCULAR ENCEPHALOPATHY WITH USING ANTIHOMOTOXIC PREPARATIONS
Dr. med. Sokolova L.I., Gorsea Ya.M., Radzhkovskaya N.S. National Medical University, Kiev municipal clinic hospital #4
Summary 32 patients (26 women and 6 men) suffering from discircular encephalopathy (cerebrovascular disease) were investigated in neuralgic departments of Kiev municipal clinic hospital №4 in 2002–2003.
The duration of the disease was less than a year in 13 patients and more than a year – in 19.
The causes of the disease were – hypertension in 5 patients, atherosclerosis – in 3 patients, combination of atherosclerosis and hypertension – in 25 patients and combination of diabetes and hypertension.
All patients were occasionally divided into two groups (16 persons in each). The main group included patients who received antihomotoxic preparations – Vertigoheel & Aesculus compositum in addition to standard therapy.
Patients of the control group received only traditional therapy.
Vertigoheel was prescribed in dosage 10 drops before the meal 3 times a day during 20 days. Aesculus compositum was applied in dosage 10 drops 20 minutes before the meal by the same scheme.
In the control group solcoseryl, piracetam, euphyllin or pentoxifylline, platyphylline, group B vitamins during three weeks course of the treatment.
Preparations Vertigoheel and Aesculus compositum showed good effectiveness in complex treatment of patients suffering from DE of I and II stage. Decreasing of the disease symptoms during the first week of the treatment and disappearance of the majority of complaints on the second-third week of the treatment was noted during the using of the preparations. It outstrips the effect of usage of the traditional therapy by a week. Including antihomotoxic preparations in the complex treatment of patients suffering from DE promoted not only the subjective improvement, but an objective positive dynamics of neurological status, normalizing of brain blood flow and improvement venous outflow according ophthalmoscopy, normalizing of vestibular disturbances of central character. Side effects were not noticed during the application of the preparations.
THE EXPERIENCE OF USING ANTIHOMOTOXIC PREPARATIONS ANGIN-HEEL AND ENGYSTOL IN THE TREATMENT OF CHILDREN SUFFERING FROM ACUTE TONSILLITIS
Prof. Dr. med. Karamiev S.A., Dr. med. Palatnaya L.A., Shapoval V.N. Bogomolets National Medical University
Summary The aim of the present study was the investigation of the effectiveness of complex antihomotoxic preparations Angin-Heel and Engystol in children with acute lacunar tonsillitis.
In clinic of children infectious diseases 30 children with age ranging from 2.5 to 14 years were examined. 15 children formed the control group and 15 – the main. The groups were comparable in age, diagnosis and heaviness of the disease.
The children of the main group in addition to the ordinary therapy received from the first day of staying in clinic Angin-Heel and Engystol according the standard scheme. Duration of the treatment was 7 days. The dosage of the preparations was 1/2 tablet for children before 3 years.
Children of the control group received ordinary treatment with antibiotics, polyvitamins, desensitizing preparations, inhalations with chlorophyllipt and ethonium.
All patients were laboratory investigated.
The effectiveness of the treatment was evaluated according to the investigation of the dynamics of clinic symptoms of the disease.
In the main group on the second day of the treatment normalizing of temperature, decreasing of intoxication manifestation was noted. Decreasing of the leucocytosis and neutrophilosis were observed on the 3–4 day of the treatment. On the second day of the treatment for the tonsils decreased and on the 3–4 day of the treatment it disappeared.
In the control group temperature normalized at the 3–5 day of the treatment, intoxication disappeared on the 3–4 day of the treatment, fur of the tonsils disappeared on the 4–6 day of the treatment.
Side effects were not noted during the treatment.
Received results allow recommending that preparations Angin-Heel and Engystol are effective medicines for the treatment of tonsillitis in children and can be used in combination with traditional allopathic therapy.
POSSIBILITIES OF ANTIHOMOTOXIC PREPARATION THYREOIDEA COMPOSITUM IN THE TREATMENT OF CHILDREN SUFFERING FROM AUTOIMMUNE THYROIDITIS
Prof. Dr. med. Zubkova S.T., Dr. med. Muz V.A. Komissarenko Institute of Endocrinology and Metabolism AMS Ukraine, Kiev
Summary Possibilities of the using of antihomotoxic preparation Thyreoidea compositum in the treatment of patients with autoimmune thyroiditis (AIT) were investigated.
Therapeutic effectiveness of preparation Thyreoidea compositum was evaluated in 20 patients in puberty suffering from hypertrophic form of AIT, mainly in condition of euthyreosis. Average age of children was 12.7 ± 1.2 years, duration of the disease was 2.0 ± 0.89 years.
Three groups of patients were chosen during the analyzing the results.
I group (10 children) were prescribed Thyreoidea compositum in dosage 1 ampoule i/m once in 3 days, 2.2 ml №10) as a monotherapy;
II group (10 patients) were prescribed complex therapy – traditional therapy with L-thyroxin (50–100 mcg) or low intensive laser influence in combination with Thyreoidea compositum, and Engystol because of frequent chronic infections.
Control group was composed with patients (19 persons) of the identical age (13.5 ± 0.45 years) who received only laser therapy or L-thyroxin in combination with laser therapy (III group).
The results of the conducted investigations allowed determining that antihomotoxic preparation Thyreoidea compositum using both in monotherapy and in complex therapy promoted the decreasing of titers antithyroid antibodies to thyroglobulin and thyroid peroxidase, regression of goiter which indicate the immunocorrective and anti-inflammatory action of the preparation.
USAGE OF ANTIHOMOTOXIC PREPARATIONS IN THE TREATMENT OF PATIENTS WITH CHRONIC HEPATITIS
Summary 24 patients suffering from chronic hepatitis (CH) against a background of chronic alcohol using were under the observation.
Chronic cholecystitis was diagnosed in 21 (28%) of patients.
Antibodies to C hepatitis of IgG class were defined in all examined patients.
Data of active viral replication were not defined, what showed the absence of the necessity of antiviral therapy.
Clinical manifestation of CH was classical: weakness, fast fatigability, discomfort in the right subcostal zone.
Laboratory investigations of functional liver samples showed the presence of cytolytic syndrome in all patients; bilirubin level was increased in 9 (37%) patients; gammopathy was defined in 12 (50%), increasing of thymol samples – in 9 patients.
Treatment included diet with higher protein and vitamin level and prescribing of hepatoprotective medicines.
On the background of diet therapy patients were prescribed antihomotoxic preparations Hepar compositum and Hepeel.
Hepar compositum was used in dosage 1 amp. i/m 2 times a week during 5 weeks. Hepeel – 1 tablet 3 times daily 15–20 minutes before the mealtime or 1 hour after.
Under the influence of the therapy all patients noted improvement of general condition, decreasing intoxication, sleep, efficiency and mood improvement.
Side effects were not revealed.
Dynamics of biochemical liver samples was positive.
Manifestation of chronic cholecystitis was noticeably decreased in all patients.
Duodenal probe showed decreasing of leucocytes, cholesterol crystals, and mucus in bile.
Thus complex use of antihomotoxic preparations in patients with CH of mixed aetiology (C viral hepatitis and alcohol) in latent period (when antiviral treatment is not indicated) is an effective method of treatment, directed for normalizing of liver and biliary system functions.
EVALUATION OF THE EFFICIENCY OF COMPLEX ANTIHOMOTOXIC PREPARATIONS GRIPP-HEEL, ENGYSTOL AND EUPHORBIUM COMPOSITUM S IN PROPHYLAXIS AND TREATMENT OF GRIPPE AND ACUTE RESPIRATORY VIRAL INFECTIONS IN CHILDREN
Summary The use of antihomotoxic preparations for prophylaxis and treatment of grippe and acute respiratory viral infections (ARVI) was studied.
In the season 2002–2003 antihomotoxic preparations Gripp-Heel and Engystol were used for prophylaxis and treatment of grippe and ARVI.
Gripp-Heel was prescribed in dosage 1 tab. 1–3 times a day sublingual 15 minutes before the mealtime or 1 hour after during a month, and then Engystol – 1 tab. 1–2 times daily during that term.
Blind random investigation was done among 42 healthy children in the age ranging from 6 to 14 years (19 boys and 23 girls). All children were divided into two groups – control and main, 21 children in each group.
Children of main group were prescribed Gripp-Heel and Engystol as a prophylaxis measure, children of control group did not receive any preparations.
Results evaluation was done by method of accidental selection with calculation of difference among frequency of indications in separate series.
The investigation has been shown that the usage of Gripp-Heel and Engystol as a prophylaxis measure 2.3 times decreases the morbidity of grippe and ARVI (p<0.05). Even though children fall ill the percentage of light and heavy forms was 28.5%, while children in control group the same data was 61.9%.
The illness is taking his normal course in the main group, whereas in the control group complications were observed in 4.8% cases (arthritis).
15 children in the age ranging from 5 months till 14 years old (8 boys, 7 girls) were observed during investigation of the effectiveness of usage antihomotoxic preparations in the treatment of grippe and ARVI.
By the aetiology ARVI were distributed consequently: grippe – 5 children, paragrippe – 3, RS-infection – 1, ARVI of unstated aetiology – 5 children.
13 children were included to the control group correlated with the main in heaviness of the disease, sex, age and diagnoses. These children were prescribed febrifuge, antihistamine preparations and vitaminous preparations.
The treatment of grippe and ARVI with Gripp-Heel and Euphorbinum compositum S accelerates the reverse development of the symptoms as sore throat, cough, headache and pain in muscles according to the results of the investigation.
Thus in children of the main group stuffy nose, headache, pain in muscles, cough disapeared quicker than the control group. Preparations were of good tolerance, did not show any side effects.
I. Introduction One of the most important functions of the skin is to protect the organism against noxae and to guarantee regulated exchange of substances between the organism and its environment. If medicaments have to be brought into the organism by the percutaneous route, then this physiological protective barrier has to be overcome.
One method of transporting active substances through the skin into deeper lying tissue or to increase the extent of normal substance diffusion is direct current therapy. Transcutaneous ion transport, known as ionophoresis, is facilitated by this. Nevertheless, a prerequisite for this is that the pharmacologically active component of the dermatic is present in an electrically charged condition. According to whether the active substance is positively or negatively charged, the medicament is applied beneath the anode or cathode.
More recent studies⁴ ⁵ demonstrate that when ionophoresis is compared with diffusion, increased substance transport takes place only in the horny layer of the horrifying squamous cell layer. Since it is just this horny layer which represents the most effective barrier against diffusion of active substances, greater effectiveness can be achieved here by ionophoresis.
However, the active substances are spread within tissue layers lying below mainly by diffusion along the concentration gradient³.
With regard to the therapeutic effectiveness of this method, a pilot study³ after iontophoretic administration of a non-steroidal antirheumatic agent, humeral epicondylopathy being indicated, revealed a significant decrease in average pain intensity in the case of tenderness and total pain sensation, but further assessment features showed only a slight improvement. However, because of the lack of a comparative group, separation of the medicinal from the physical therapy effect was not possible.
In the case of ointments or gel preparations which contain only one medicament with positive or negative charge, substance transport of greater extent with the aid of direct current is evident because of conformity with natural physical laws¹. The therapeutic effectiveness of a combination treatment of direct current/medicament is also documented empirically elsewhere².
In the case of pharmaceutical mixtures, as are present in phytotherapeutic extracts and homeopathic preparations, it is not known as a rule whether the effective constituents are present in ionized form and if so, what charge they have. In addition there is the fact that it must be assumed in the case of these medicaments that several constituents which can also have different electrical charges are therapeutically effective.
The user can change the current direction at the iontophoresis unit in the course of therapy in order to be able to let both the positively and the negatively charged constituents through the skin into the tissue. Nevertheless, electrically neutral substances cannot be transported more quickly into foreign tissue by this method.
The objective of this investigation was to ascertain whether the combination of a Traumeel ointment therapy with iontophoresis has a better therapeutic result, i.e., faster restoration of health, than application of ointment alone. The therapeutic effectiveness of Traumeel ointment in distortions has been proven without doubt in the course of a double blind study⁶. Taking this effectiveness as proven, the therapeutic comparison of Traumeel ointment versus Traumeel ointment/direct current therapy was sufficient for us in this study without inclusion of a placebo.
II. Patients and methodology
A total of 50 patients with medium degree injuries were included in the study. All had the same type injury of external ligamentous overstretching in the sense of supination distortion trauma. 25 patients were treated exclusively with Traumeel ointment. The other 25 patients were subjected in addition to direct current therapy.
After the injury, immobilization in a Traumeel ointment dressing was provided for two days for all patients. No further dressings were applied after this.
One group of patients received following this a physiotherapy every 2 days in the shape of iontophoresis with a current intensity of 3 mA for a period of 10 minutes per session. The ointment was applied alternatingly for each patient both on the cathode and on the anode. Cold packs were applied in each case following this treatment. Traumeel ointment for daily self-application was prescribed to the patients of the other group. The patients were examined on the day of injury as well as on the 1st, 3rd, 5th, and 7th day. Assessment criteria were pain at rest, under pressure, and in motion, and were documented by means of a 4 point scale (0 = without, 1 = little, 2 = medium, 3 = severe). Furthermore, the circumference was measured with the aid of a tape measure over the narrowest point, the ankle, and the metatarsus. The mobility of the ankle joint was measured according to the neutral zero method. Circumference and mobility were compared with the healthy side in each case and the change in difference was evaluated. Since the patients were competitive athletes, the period up to the first day of return to athletic training was taken as the criterion for assessing the therapy.
III. Results
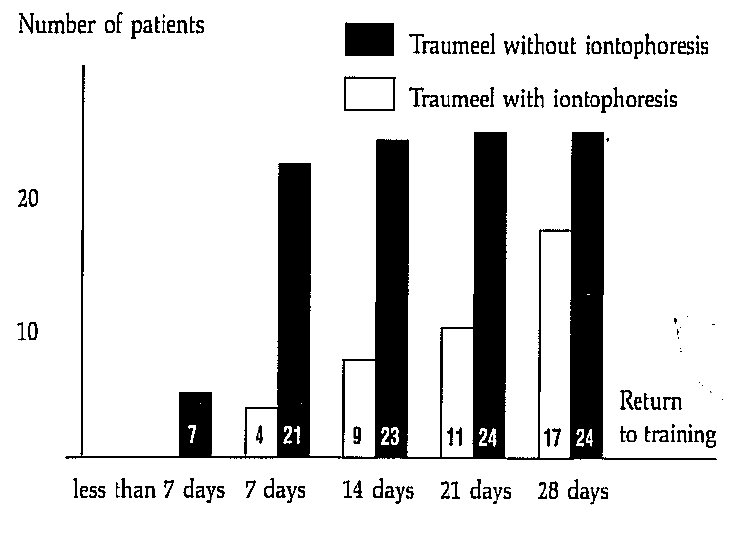
1. Return to training If the two groups are compared with one another with regard to the first day of return to training, it results that more patients in the group treated solely with Traumeel ointment returned to training at an earlier point in time.
Fig. 1: Return to Training
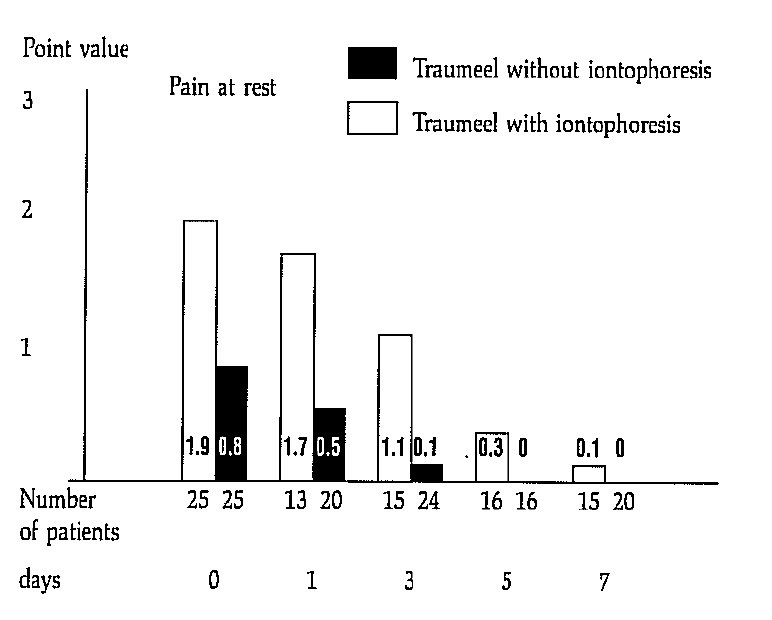
2. Pain at rest Fig. 2: Course of the average pain at rest values
The intensity of the pain at rest was documented in the shape of point values on the 1st, 3rd, 5th, and 7th day of treatment.
The starting value of the two groups were different (with iontophoresis 1.9; without iontophoresis 0.8), so that a comparison of the course with regard to this feature could be made only conditionally. However, it can easily be seen from Figure 2 that both starting values decreased over the 7 days continuously and in a comparable ratio. In the group treated only with ointment, the value of 0.1 was reached for pain at rest within 3 days because of the low starting value; in the iontophoresis group, this value was reached only on the 7th day. (However, the higher starting values existed here.)
Since various patients did not appear at some appointments for “nonmedical reasons”, the starting values of these dropping out patients were analyzed separately. Since these were not extreme values, the average trend values of the assessment features were not distorted by the lack of these data.
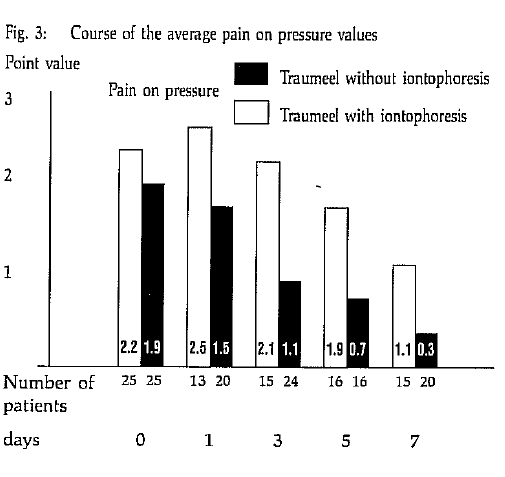
3. Pain on pressure
Fig. 3: Course of the average pain on pressure values
The starting values in both groups were comparable with regard to this feature (iontophoresis group on average 2.2; Traumeel group on average 1.9). The intensity of pain on pressure also decreased here continuously as can be seen in Figure 3 from 1.9 points to 0.3 points. In the iontophoresis group, the average pain intensity increased at the beginning (from 2.2 to 2.5) and then decreased continuously but significantly slower than in the Traumeel group. On the 7th day of observation, an average residual pain on pressure of 1.1 was still present.
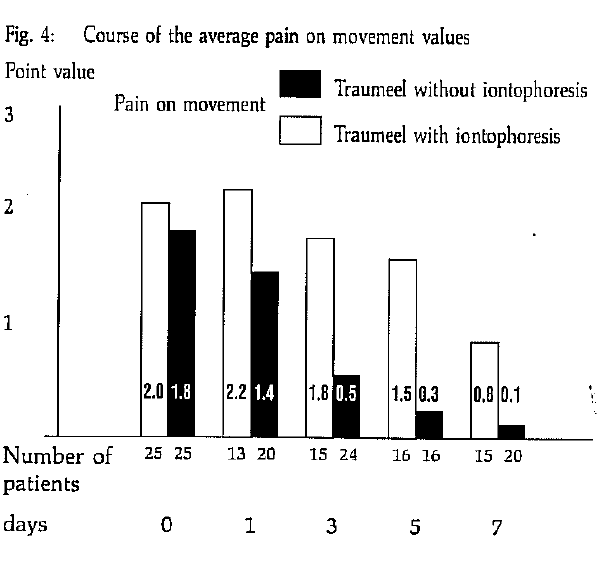
4. Pain on movement Fig. 4: Course of the average pain on movement values
The starting values of both groups were also comparable in the case of this feature (iontophoresis group on average 2.2; Traumeel group on average 1.9). The intensity of pain on movement also decreased here continuously as can be seen in Figure 4 from 2.0 points to 0.3 points.
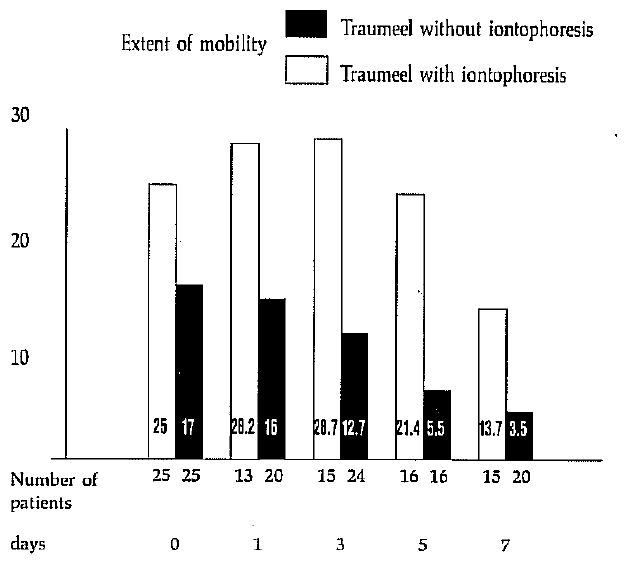
5. Mobility The mobility of the healthy and injured joint was measured according to the neutral zero method and the difference between the two values was formed.
In the Traumeel group, this difference decreased to the value of 3.8° on the 7th day, a negligible value, which lies in the range of the error limits. In the iontophoresis group, a residual angle difference of 10.7° remained on the 7th day after initial deterioration (Fig. 5).
Fig. 5: Course of the average extent of mobility (Difference between injured and healthy joint)
6. Circumferential measurements The data of the circumferential measurements are only conditionally suitable for interpretation (see discussion), since the spread (see table 1) and the value range are too large.
IV. Discussion In orthopedic traumatology, there is a trend towards treating the consequences of injury with antiphlogistic ointments and to make therapeutic use of the stimulating effect of direct current treatment (galvanization). The ionization of the active substance is considered to be secondary.
As can be seen from the above tables, an increase in swelling in the ankle joint region was noticed in the control examinations in the iontophoresis group. This is attributable to a condition of irritation caused by electrotherapy as well as to sacculation of the hematoma of the distal joints of the metatarsus.
On critical comparison of the two forms of application of iontophoresis and simple treatment with ointments after inital elastotape dressing, the latter musgt be given preference because of the more rapid incidence of effect, in particular for competitive athletes. Exclusive ointment application has also the advantage of being free of irritation. Side effects were not observed in any patient.
On the other hand, iontophoresis has proven itself for patients who cannot tolerate adhesive dressings for several days (lacing effect in varicosis) or who themselves cannot rub in ointments for certain reasons (older people, disabled etc.). Application of ointment alone, i.e. without initial tape dressings, should be performed only for simple bagatelle injuries which require no specific medical supervision.
Literature
Pratzel, H., Die Iontophorese, Med.-Info Nr. 1 (Transcutan GmbH)
Magyarosy, J., Ernst, E., Marr, N., Schmolzl, Ch., …
Schops, P., Seichert, N., Erdl, R., Siebert, W., Pratzel, H., Pilotstudie zur klinischen Wirksamkeit einer definierten Iontophorese mit Indometacin bei Epicondylopathia humeria, Z. Phys. Med. Baln. Klin. 15, 395–399 (1986)
Pratzel, H., Grundlagen des perkutanen Stofftransports in der Pharmako-Physio-Therapie und Balneotherapie, Dissertation 1985 (quoted in 3)
Pratzel, H., Machens, R., Dittrich, P., Iontophorese zur forcierten Hautresorption von Indometacin und Salicylsaure, Z. Rheumatol. 104, 40, 748 (1986) (quoted in 3)
Zell, et al., publication in preparation
Address of the author: Dr. med. Werner Thiel Orthopedic physician Kirchstraße 9 D‑6635 Bous Germany
Reprinted from Biologische Medizin (1999 Feb) 1:4–8.
Abstract
This study investigates whether the effects of cAMP Injeel® and cAMP Injeel® forte in a cell-free system are unique to these preparations or simply equal the additive effects of their single-potency components. When one of the single-potency components of cAMP Injeel® and Injeel® forte was selected as a base potency and the others were added in succession, recorded enzyme activity correlated with the number of potencies added. In all cases, the inhibiting effect of mixed potencies was greater than that of the single potencies, but in no case did the level of inhibition produced by a mixture equal the sum of the effects of its single-potency ingredients.
Introduction
Potency chords are mixed-potency preparations containing equal portions of three potencies of the same substance—a base potency and two additional levels. These potency chords are available commercially under the trade name Injeel®. The “forte” variation includes four rather than three different potencies.¹
The authors confirm the results of the animal experiments reviewed in the article on potency chords in Volume 6/98 of Biologische Medizin (Franke W: Efficacy of Homeopathic Dilutions in the Form of Potency Chords. J Biol Med. 1998;27(6):276–278). The work of the authors on the effects of single and mixed potencies of cAMP on acid phosphatase activity offers additional impressive proof (probability of error 1%; p < 0.01) that potency chords are superior to single potencies in efficacy.
Hartmut Heine, Ph.D.
Materials and Methods
Active Agents
The active substance cAMP was used in the following forms: 6X, 12X, 30X, 200X, cAMP Injeel® (12X/30X/200X), and cAMP Injeel® forte (6X/12X/30X/200X). All preparations were used in liquid form and were supplied in 5 ml ampules by Biologische Heilmittel Heel GmbH, Baden-Baden. (Please note that these cAMP Injeels® are not available commercially.) All cAMP potencies, as well as the Injeel® and its Injeel® forte variation, were produced according to homeopathic principles. The study utilized a blind test format; all preparations were coded prior to use but decoded prior to statistical analysis.
Chemicals
The synthetic enzyme substrate p-nitrophenyl phosphate was supplied by Serva of Heidelberg (Cat. # 30770). All other chemicals used were of the highest available degree of purity.
Enzyme Test System
The enzyme used was acid phosphatase (AP) derived from potatoes (Boehringer, Mannheim; Cat. # 108197). This enzyme model is biologically relevant because acid phosphatase occurs naturally in the lysosomes of human cells. For use in the experimental setups, the enzyme was diluted 1 : 200 with 10 mM of NaAc (pH 5.6).
Incubation Technique
The catalytic activity of AP was measured by determining the amount of p-nitrophenol formed in a microtiter plate assay. 20 µl of the enzyme suspension (out of a total volume of 120 µl) and the cAMP preparation being tested (or water, in the case of the control) were preincubated together at 30 °C. Two series of assays were performed. In one, the preincubation period was 20 minutes; in the other, 40 minutes. After preincubation, each batch of assay components was mixed with 100 µl of the synthetic substrate (5.5 mM p-nitrophenyl phosphate in 0.1 M citrate buffer, pH 5.6) and reincubated at 30 °C. After five minutes, the reaction was stopped by adding 100 µl of 1 N NaOH, and the quantity of enzymatically formed p-nitrophenol was determined using a temperature-controlled microtiter plate reader (ATT C 340, SLT Instruments, Crailsheim) at a wavelength of 405 nm.
The quantity of p-nitrophenol was determined by applying the reference equation p-nitrophenol [nmol × ml⁻¹] = 64.82 × OD 405 nm – 3.373; correlation coefficient 0.998. p-nitrophenol in various concentrations served as the reference substance.
Figure Captions
Fig. 1: Activity of acid phosphatase (AP) in the presence of different cAMP preparations. The graph presents average values (± standard deviation). The line segment ending in circles represents the control. Statistics (n = 48): All experimental mixtures differed significantly from the control (p < 0.01), and 12X differed significantly from all mixtures (p < 0.01). To show the linear relationship among the values more clearly, the y axis begins at 4 instead of at 0, and a line has been drawn connecting the average values for 12X and the Injeel®. The table below the graph shows the composition of the experimental mixtures.
A) Graph (reproduced qualitatively)
(The original plotted mean AP activity [nmol · min⁻¹ · ml⁻¹] ± SD for each setup, y-axis running from 4–10, control marked by ●, and a trend line connecting 12X → Injeel®.)
B) Assay‐Component Table
Component →
12X
12X / 30X
12X / 30X / 200X
Injeel® (12X/30X/200X)
12X
25 µl
25 µl
25 µl
75 µl
30X
–
25 µl
25 µl
–
200X
–
–
25 µl
–
Injeel® stock*
–
–
–
25 µl
Water
75 µl
50 µl
25 µl
25 µl
Enzyme (AP)
20 µl
20 µl
20 µl
20 µl
*In the “Injeel®” column this refers to the mixed‐potency stock (12X / 30X / 200X).
Fig. 2: Activity of acid phosphatase (AP) in the presence of different cAMP preparations. The graph presents average values (± standard deviation). The line segment ending in circles represents the control. Statistics (n = 48): All experimental mixtures differed significantly from the control (p < 0.01), and 30X differed significantly from all mixtures (p < 0.01). To show the linear relationship among the values more clearly, the y axis begins at 4 instead of at 0, and a line has been drawn connecting the average values for 30X and the Injeel®.
A) Graph
(Original mean ± SD plot, y-axis 4–10 nmol·min⁻¹·ml⁻¹, control ●, trend line connecting 30X → Injeel®.)
B) Assay-Component Table
Component →
30X
30X / 200X
30X / 200X / 12X
Injeel® (12X/30X/200X)
30X
25 µl
25 µl
25 µl
–
200X
–
25 µl
25 µl
–
12X
–
–
25 µl
–
Injeel® stock*
–
–
–
75 µl
Water
75 µl
50 µl
25 µl
25 µl
Enzyme (AP)
20 µl
20 µl
20 µl
20 µl
Fig. 3: Activity of acid phosphatase (AP) in the presence of different cAMP preparations. The graph presents average values (± standard deviation). The line segment ending in circles represents the control. Statistics (n = 48): All experimental mixtures differed significantly from the control (p < 0.01), and 200X differed significantly from all mixtures (p < 0.01). To show the linear relationship among the values more clearly, the y axis begins at 4 instead of at 0, and a line has been drawn connecting the average values for 200X and the Injeel®. The table below the graph shows the composition of the experimental mixtures.
A) Graph
(Original mean ± SD plot, y-axis 4–10 nmol·min⁻¹·ml⁻¹, control ●, trend line connecting 200X → Injeel®.)
B) Assay-Component Table
Component →
200X
200X / 12X
200X / 12X / 30X
Injeel® (12X/30X/200X)
200X
25 µl
25 µl
25 µl
–
12X
–
25 µl
25 µl
–
30X
–
–
25 µl
–
Injeel® stock*
–
–
–
75 µl
Water
75 µl
50 µl
25 µl
25 µl
Enzyme (AP)
20 µl
20 µl
20 µl
20 µl
*In the “Injeel®” column this refers to the mixed-potency stock (12X / 30X / 200X).
Setup
Composition
Volumes Added
1
6X
25 µl cAMP 6X + 75 µl water
2
6X / 12X
25 µl 6X + 25 µl 12X + 50 µl water
3
6X / 12X / 30X
25 µl 6X + 25 µl 12X + 25 µl 30X + 25 µl water
4
6X / 12X / 30X / 200X
25 µl 6X + 25 µl 12X + 25 µl 200X + 25 µl water
5
Injeel® forte
100 µl Injeel® forte stock (6X/12X/30X/200X)
6
Control
100 µl water
Fig. 4: Activity of acid phosphatase (AP) in the presence of different cAMP preparations. The graph presents average values (± standard deviation). The line segment ending in circles represents the control. Statistics (n = 48): All experimental mixtures differed significantly from the control (p < 0.01), and 6X and 6X/12X differed significantly from Injeel® forte (p < 0.01). To show the linear relationship among the values more clearly, the y axis begins at 4 instead of at 0, and a line has been drawn connecting the average values for 6X and the Injeel® forte. The table below the graph shows the composition of the experimental mixtures.
A) Graph
(Original mean ± SD plot, y-axis 4–10 nmol·min⁻¹·ml⁻¹, control ●, trend line connecting the series 6X → Injeel® forte.)
B) Assay-Component Table
Component →
6X
6X / 12X
6X / 12X / 30X
6X / 12X / 30X / 200X
Injeel® forte (6X/12X/30X/200X)
6X
25 µl
25 µl
25 µl
25 µl
–
12X
–
25 µl
25 µl
25 µl
–
30X
–
–
25 µl
25 µl
–
200X
–
–
–
25 µl
–
Injeel® forte stock*
–
–
–
–
100 µl
Water
75 µl
50 µl
25 µl
25 µl
–
Enzyme (AP)
20 µl
20 µl
20 µl
20 µl
20 µl
*In the “Injeel® forte” column, this refers to the mixed-potency stock (6X / 12X / 30X / 200X).
Statistics
The measured values obtained for all setups (activity per volume in nmol × min⁻¹ × ml⁻¹) were subjected to single-factor variance analysis (ANOVA). Subsequently, the Fisher LSD test was performed to directly compare the effect of the control to that of each cAMP preparation or stage in the additive series of cAMP potencies. A probability of error of 1% (p = 0.01) was chosen as the limit of significance.
Results and Discussion
cAMP Injeel®
The cAMP Injeel® used in these experiments is a 1 : 1 : 1 mixture of the single potencies 12X, 30X, and 200X. In numerical terms, adding 75 µl of this mixture to a setup adds 25 µl each of 12X, 30X, and 200X. The design of our experiments took this fact into account, as exemplified by Series 1 (Figure 1):
Setup 1 (12X) contained 25 µl of cAMP 12X and 75 µl of water.
Setup 2 (12X/30X) contained 25 µl each of 12X and 30X, plus 50 µl of water.
Setup 3 (12X/30X/200X) contained 25 µl each of 12X, 30X, and 200X.
Setup 4 (Injeel®) contained 75 µl of cAMP Injeel® and 25 µl of water.
Control contained 100 µl of water.
Each setup was mixed with 20 µl of AP suspension and preincubated at 30 °C. After 20 minutes, 100 µl of the substrate solution were added and incubation was continued for five more minutes. The reaction was then stopped and the quantity of enzymatically formed p-nitrophenol was determined through spectrophotometry.
As Figure 1 shows, all cAMP preparations inhibited the catalytic activity of AP. A linear decrease in enzyme activity is apparent in the series 12X → 12X/30X → 12X/30X/200X → Injeel®. A similar tendency was observed both when 30X was chosen as the base potency and 200X and 12X were added one at a time (Figure 2), and when 200X was chosen as the base potency and 12X and 30X were added (Figure 3).
A linear decrease in AP activity was also apparent when the preincubation period was increased from 20 to 40 minutes. Inhibition of AP was more moderate, however, and the recorded values were different (data not shown).
cAMP Injeel® forte
cAMP Injeel® forte is a mixed potency consisting of equal parts of the single potencies 6X, 12X, 30X, and 200X; thus, 100 µl of this mixture contains 25 µl each of 6X, 12X, 30X, and 200X. See the table for the components and test sequence leading to the Injeel® forte variant.
The experiments were conducted in the same way as the Injeel® experiments. As Figure 4 shows, all of these cAMP preparations inhibited AP catalytic activity. A linear decrease is again apparent in the series leading from 6X to the Injeel® forte. The same phenomenon is apparent when 12X, 30X, or 200X is chosen as the base potency (data not shown).
From these results, we can conclude that the effects of cAMP potency chords are not identical to the sum of the effects of the individual potencies they contain. As this example shows, potency chords such as Injeel® or Injeel® forte preparations seem to have qualitatively new and unique effects. Further investigation will be needed in order to determine whether this conclusion also applies to Injeel® and Injeel® forte preparations of other substances.
References
Wissenschaftliche Abteilung der Firma Biologische Heilmittel Heel GmbH. Ordinatio Antihomotoxica et Materia Medica. Baden-Baden. 1996:13.
Stryer L. Biochemie. 4. Auflage. Heidelberg: Spektrum. 1996:779–802.
Harisch G, Dittmann J. Untersuchungen zur Wirkung von Ubichinon-Injeel und Injeel forte mit zellfreien Systemen. Biol Med. 1997;26(3):99–104.
Harisch G, Dittmann J. Einfluss von cAMP-Potenzen auf die katalytische Aktivität der Sauren Phosphatase. Erste Hinweise für divergierende Wirkungsqualitäten von Einzelpotenzen und Potenzmischungen. Biol Med. 1998;27(5):212–219.
For the authors
Joachim Dittmann, Ph.D. Institute for Physiological Chemistry Veterinary College of Hannover P.O. Box 71 11 80 D-30545 Hannover Germany
BioMedical Therapy Magazine Symposium At the Royal Society of Medicine, London 10. 5. 1997
A. Introduction
Although the use of corticosteroids is accepted as a standard technique in the treatment of several inflammatory diseases, we must recognize that specific injection techniques of anti-inflammatory products are gaining more and more interest. Most physicians, however, tend to regard these techniques as marginal phenomenons. The importance of these injections in the treatment of so-called inflammatory diseases is relatively unexplored and promises to be a fertile area for further investigation. Since most physicians have never been trained in these techniques, they are anything but expert in this field. I think that every therapist should at least know about the existence of this strategy, even if he or she will not use injections in his or her own practice. So, I will introduce to you today the therapeutical strategies that focus on injections of non-steroid products. Both chemotherapeutic and biotherapeutic products will be discussed, and several techniques of administrating them will be explained. The clinical cases will try to illustrate my strategies. I have more than ten years of experience with these techniques in my private practice as a general practitioner in Belgium, and I have noticed that there is a very broad spectrum of medical problems that can be managed with this injection strategy. Today, however, I will only discuss two examples of alternatives for cortisone: the treatment of musculoskeletal pain and the treatment of asthma. Still, I do not make any claims about the injections described in this lecture, involving the prevention or cure of any disease. Maybe the effects that I have noticed in my private practice are no more than a sophisticated placebo. I cannot be sure that what I am doing is best for the patient unless this practice has been rigorously tested; to check the items that I suggest, large-scale clinical studies are necessary. This lecture can be regarded as an invitation to do so in the near future.
B. Injection of biotherapeutics
B.1. Injection of biotherapeutics is not a very strategic novelty
Those familiar with biotherapeutics for injection know that many ampoules exist since several decades, especially in Germany. Especially Heel, Pflüger, Steigerwald, Dolisos, Cosmochema, Fides and Hevert are famous for their ampoule preparations. Thousands of them are injected every day, and clinical studies check their efficiency and control their possible side-effects (ref. 20, 21, 28, 29). A wide selection of homeopathic and phytotherapeutic preparations has been on the market in injection form for many years now, and they have been employed in daily medical practice with good success, especially by general practitioners, rheumatologists and orthopaedic doctors. Many authors have already mentioned the use of biotherapeutic ampoules for injection: Bianchi (ref. 3), Claussen (ref. 13), Coeugniet, de La Fuye (ref. 31), Diamond (ref. 44, 45), Fischer (ref. 36), Frase, Gellman (ref. 19), Graf von Ingelheim (ref. 27), Geyer (ref. 24), John, Kleinscholt, Küstermann, Lannugier-Bolling, Meltelmann (ref. 28, 29), Müller, Pollmann, Potrafki (ref. 21), Preusser, Reckeweg (ref. 14), Riley (ref. 16), Risch, Schmid (ref. 17), Subotnick (ref. 43, 48), Thiel (ref. 20), Timmermann (ref. 10), Vorstoffel (ref. 33), Wachter, Werthmann, Weiser (ref. 28), Zenner (ref. 29) and many others (see ref. 1: bibliography). Since there was no specific name for all the methods that use biotherapeutics for injection on specific spots, I introduced in Belgium the term ‘biopuncture’ (ref. 1, 2, 5), in order to distinguish the use of homeotherapy according to de La Fuye (ref. 31), neural therapy according to Huneke (ref. 11), ampoules over nerve blocks according to Bracho (ref. 12) and segmental acupuncture according to Pistor (ref. 32). At the same time we want to give more credibility and respect to orthodox doctors as to therapists in natural medicine (ref. 1, ref. 8). In this way, we shall stimulate its use, so that the strategy of using these injections is developed in everyday practice. Let us now go a little deeper:
C. Biotherapeutics for local injections?
C.1. Subcutaneous injection
One of the most familiar ways of using biotherapeutics in everyday practice. Most of you use them in the oral form, as tablets or drops. Although you may not be interested in giving injections in your practice, I think it is good to know more about the enormous possibilities of these biotherapeutic drugs. And it might give you a broader view on natural medicine, because injections can act in a more powerful way than oral medication. The exact choice of the remedy itself (ref. 1, 2, 5).
C.2. Acupuncture point injections
Those doctors familiar with acupuncture, can enhance their therapeutic effect by injecting intracutaneously or subcutaneously a biotherapeutic product instead of dry needling. This method was mentioned before by de La Fuye, Geyer, Matz, Frase and many other authors. It is theoretically possible to inject a single remedy into an acupuncture point that is known for certain indications. This combination of homeopathy and Chinese medicine (homoeosinaty) was introduced by de La Fuye. I will give you some examples:
Chelidonium on Liver 13 for drainage of the liver, Nux Vomica on Bladder 21 for gastritis, Gnaphalium on Bladder 34 for ischias, Sulfur on Bladder 52 for eczema, Cantharis on Kidney 11 for cystitis, Lobelia on Kidney 27 for asthmatic bronchitis, Naja Tripudians on Bladder 17 for cardiac neurosis, Crataegus on Heart 3 for palpitations, Thuja on Gallbladder 30 for coxarthrosis, Echinacea on Jenn Mo 19 for cough, asthma, bronchitis Echinacea on Jenn Mo 22 (for cough, asthma, bronchitis), Lachesis on Small Intestine 19 for vertigo, Sulfur on Bladder 31 for climacteric disorders.
Cralonin on Heart 3 for palpitations, Cralonin on Bladder 15 for palpitations, Engystol on Small Intestine 14 for asthma, Vertigoheel on Small Intestine 19 for vertigo, Mullein pro injectione on Urinary Bladder 31 for climacteric disorders, Traumeel on Gall bladder 20 for headache, Spigelon on Gall bladder 20 for headache, Zeel on Gall bladder 30 for pain in the hip region, Pulsatilla composition on Jenn Mo 6 for activation of the defensive system.
It is also possible to inject a complex remedy into several points of an acupuncture meridian, like for example Discus compositum over the Governor vessel. Subcutaneous or intracutaneous injections are given on the mid-line of the back, or at the level of every vertebra in the region of the pain. Those allopathic products should always be used in a diluted way (half a normal dose, adding several ml of physiological fluid and several ml of a local anesthetic), and should be injected with more care than the biotherapeutic one. I use them as a replacement for corticosteroid injections (see also ref. 51). Of course, some injections are given at the physician’s own responsibility, when the product is used in a way for which it has not been registered. Ticlodil is officially designed for the intravenous/intramuscular injection only and an oral Feldene is officially designed for the intramuscular injection only. So, I can not make any claims about their safety and efficacy, until more large-scale clinical studies are performed.
F. Is it always necessary to give injections?
For those therapists who are not allowed to give injections, I can recommend to do trigger point therapy with stretch and spray, as Travell and Simons suggest. This is an easy and safe technique, and gives interesting results when dealing with several myofascial disorders. The patient is usually very enthusiastic, since he or she has almost immediate relief. Although this effect is temporary, long term effects are achieved with repeated sessions. Even more interesting is ischemic compression. Ischemic compression is application of progressively stronger, painful pressure on a trigger point for the purpose of eliminating the trigger point’s tenderness and hyperirritability. Similar to acupressure and shiatsu, the thumb is used as the therapeutic tool. But we do not deal with acupuncture points, but solely with active trigger points, which can be found by clinical examination. The thumb action blanches the compressed tissues, which usually become flushed (hyperemic) on release of the pressure. The use of Traumeel ointment during and after the compression, enhances the effects of the treatment. The clinical effects of the technique depend largely on the skills of the therapist. When looking for the active trigger points, wall plates can help. Textbooks (by Baldry, Travell and Simons) give more fundamental information on this subject. In Belgium, I am giving workshops on trigger point therapy, in order to show how this technique can be performed in everyday practice.
Case:
Clinical examination shows a painful zone in the right brachioradialis muscle and a small spot at the epicondylus radialis, that is painful on digital pressure. He had ischemic compression on two trigger points in the brachioradialis muscle, twice a week. He also got a local application of Arnica comp. ointment (e.g. Traumeel) in the right brachioradialis muscle and on that small painful spot at the epicondylus radialis, three times a day. Additional oral treatment with Ferrum-Homaccord, ten drops three times daily, gave complete relief after two weeks.
Case:
A girl of twelve has suffered a contusion of the lateral part of the thigh while snowboarding. The examination on the evening shows an obvious swelling of the thigh and an extensive haematoma. The region is very sensitive to pressure, and she refuses a local injection. I give her Arnica comp. ointment (Traumeel ointment, which was cooled in the fridge) and she applied it every hour the first day, every two hours the second and third day and four times a day the three next days. Putting the ointment in a refrigerator before application gives an extra cooling down in an acute situation. As an additional therapy, she received Arnica comp. tablets: I told her to take them at the same frequency as the application of the ointment. I asked her to keep the tablets in the mouth as long as possible, to give the product maximum resorption via the oral mucosa. After six days the pain and swelling were completely gone.
G. Conclusion
Although the use of corticoids is accepted as a standard technique in the treatment of several inflammatory diseases, we must recognize that specific injection techniques of biotherapeutic products are gaining more and more interest. Most physicians, however, are not familiar with these techniques. That is why I wanted to show the importance of these injections in the treatment of so-called inflammatory diseases. By using biotherapics (drops or tablets), I have experienced that the combination of oral application (drops or tablets) and local treatment (ointment and/or injections) gives interesting results, both in acute as in chronic cases.
Kersschot, J., Biopuncture and antihomotoxic medicine Aartselaar, inspiration ed., 1997
Timmerman, J., Clinical Evidence of the Efficacy of a Homeopathic Medication for the Intervertebral Treatment of Lumbar and Cervical Pain Unpublished Report (Biological Therapy)
Dosch, P., Manual of neural therapy according to Huneke Haug Publishers, 1984
Bonica, J., Clinical applications of diagnostic and therapeutic nerve blocks Springfield, Charles C Thomas Publisher, 1959
Claussen, Claus-F., The Homotoxicology, the core of a Probiotic and Holistic Approach to Antioxidant Medicine Biologische Medizin 1993; 1: 21-23
Risch, K.–H., Behandlung der Gonarthrosen mit Zeel Injektionslösung – Ergebnisse einer Anwendungsbeobachtung Biologische Medizin, Heft 4, August 1993, 193-201
Ricken, K.–H., Die chronische Polyarthritis und andere immunologische Erkrankungen – eine Domäne der antihomotoxischen Therapie? Biologische Medizin, 24. 3, 142-149, Juni 1995
Riley, D., An Introduction to Homotoxicology Albuquerque, Menaco Publishing, 1990
Schmid, F., et al Antihomotoxische Medizin, Band I: Grundlagen, Klinik, Praxis; Band II: Homöopathische Antihomotoxika Baden-Baden, Aurelia-Verlag, 1996
Baldry, P., Acupuncture, Trigger Points and Musculoskeletal Pain New York, Churchill Livingstone, 1989
Gellman, H., Complementary Therapy for the Treatment of lateral epicondylitis and stenosing tenosynovitis Unpublished Report (Biological Therapy)
Thiel W., Borho, B., Die Therapie von frischen, traumatischen Blutergüssen der Kniegelenke (Hämatrhos) mit Traumeel Injektionslösung Biologische Medizin, April 1991, nr.2, 506-515.
Potrafki, B., Degenerative Erkrankungen des Knies und ihre Behandlung mit Zeel Biologische Medizin, Augustus 1993, nr.4, 230-231.
Matusiewicz, R., Wirksamkeit von Engystol N bei Bronchialasthma unter kortikoidabhängiger Therapie Biologische Medizin 1995 (5), 242-246
Vosgrau, M., Grundlagen und Ergebnisse der Therapie mit Potenzakkorden Homotox-Journal, 1970, 9e Jg., nr. 6, p.135-143.
Geyer, E., Praktische Homöopathie und Akupunktur Karlsruhe, DHP
Rubin, D., Myofascial trigger point syndromes: an approach to diagnosis and treatment Biological Therapy 1994; 2: 90-91
Werthmann, K., Antihomotoxische Therapie der viszeralen Erkrankungen Biologische Medizin 1993; 1: 26-29
Zenner, S., Behandlung der Gonarthrose mit Zeel P Injektionslösung – Ergebnisse einer Anwendungsbeobachtung Biologische Medizin, Heft 4, August 1993, 193-201
Wesler, M., Metelmann, H., Application Possibilities of Traumeel S Injection Solution: Results of a Multicentric Drug Monitoring Trial Conducted on 3,241 Patients Biological Therapy, Volume X No. 4, October 1992
Zenner, S., Metelmann, H., Application Possibilities of Traumeel S Injection Solution Biologische Medizin 1996; 3: 107-112
Melzack, R., Stillwell, D., M., Trigger points and acupuncture points for pain: correlations and implications Pain, 1977; 3: 3-23
de La Fuye, R., L’Acupuncture moderne pratique. Synthèse de l’acupuncture et de l’homéopathie Paris, Librairie E. Le François, 1976
Pistor Un défi thérapeutique: la mésothérapie Paris: Maloine, 1974
Vorstoffel, E., Therapie von Wirbelsäulensyndromen mit paravertebralen Traumeel-Infiltrationen Münch. med. Wschr. 113, 12,(1971), 440.
Tirscher H, Eder M, Infiltrationstherapie Stuttgart: Hippokrates, 3° Aufl. 1996
Bruns, J., Injuries and disabilities caused by chronic and excessive sports-related strain Biological Therapy 1993; 1: 18-20
Fischer J, Biological therapy of rheumatic pain in an orthopedist’s practice Biological Therapy 1993; 1: 31-32
Saal J S, Saal A J, Yurth E., Nonoperative Management of Herniated Cervical Intervertebral Disc With Radiculopathy Spine 1996; 16: 1877-1883
Conroy J M, Ginsberg F, Léon M, Bernard V, Appelboom T, Haazen L, Peri-articular injection of Tenoxicam for painful shoulders: a double-blind, placebo-controlled trial J Rheumatol 1993; 20: 1837-1841
Melzack R, Cibson C.Z, Simons L S, Trigger point therapy and referred pain Pain 1981; 6: 589-603
Fairbank J C T, Park W M, McCall I W, O’Brien J P, Apophyseal injection of local anesthetic as a diagnostic aid in primary low-back pain syndromes Spine 1981; 6: 598-605
Hong C-Z, Hsueh T C, Yu S, Recurrent myofascial trigger points related to traumatic cervical disc herniation Myopian San Antonio, Texas, august 1995 (third world congress on myofascial pain and fibromyalgia)
Gunn C C, Milbrandt W E, Tennis elbow and acupuncture, Am J Acupuncture 1977; 5: 61-66
Subotnick I, Overuse Injuries of the Knee and Leg Biological Therapy 1993; 2: 57-60
Diamond W J, Clinical Grand Rounds – Salmonellosis Biological Therapy 1993; 3: 90-93
Diamond W J, Clinical Grand Rounds – Energetic Presentations of Viral Disease Biological Therapy 1994; 3: 219-223
Werthmann K, Antihomotoxische Therapy of Disorders of the Stomach and Small Intestine in Pediatrics Biological Therapy 1994; 4: 262-265
Lanninger-Bolling D, Rheumatoid Disorders and their Antihomototoxic Therapy Biological Therapy 1995; 4: 131-135
Subotnick I, Sports and exercise injuries Berkeley: North Atlantic Books 1991
Schmid F., Biological Medicine Baden-Baden: Aurelia Verlag 1991
Rich B, Mc Keag D, When sciatica is not disk disease Physician and Sportsmedicine 1992; 20 (10): 105-115
Kersschot, J., Biopuncture bij lage rugpijn Arts en Alternatief 1996; 1: 12-13
Kersschot, J., Alternatives to the use of cortisone Antwerp, Congress movement counselors; 22.3.1997
Potrafki B, Sports injuries and the possibility of their antihomotoxic therapy Biological Therapy 1993; 1: 9-14
Kersschot J, The use of trigger point injections for low back pain Workshop injuistingen, Gent (Belgium): 18. 2. 97
Kersschot J., Alternatives to the use of cortisone Antwerp, Congress movement counselors; 22.3.1997
Matusiewicz, R., Traumeel S in der Behandlung von kortikoidabhängigen Bronchialasthma Biologische Medizin 1996; 3: 107-112
Zenner, S., Metelmann, H., Application Possibilities of Traumeel S Injection Solution: Results of a Multicentric Drug Monitoring Trial Conducted on 3,241 Patients Biological Therapy 1992; 4
Zell, J., Conrert, W. D., Mau, J., Feuerstake, G., Behandlung von akuten Sprunggelenksdistorsionen. Doppelblindstudie zum Wirksamkeitsnachweis eines homöopathischen Salbenpräparats, Fortschritte der Medizin 1988; 106: 96.
Gottlieb, N. L., Riskin, W., G., Complications of local corticosteroid injections JAMA 1980; 243: 1547-1548
Fitzgerald, R. H., Jr., Intrasynovial injection of steroids: uses and abuses Mayo Clin. Proc. 1976; 51: 655-659
Matusiewicz, R., Wirksamkeit von Engystol N bei Bronchialasthma unter kortikoidabhängiger Therapie Biologische Medizin 1995 ;5: 242-246
Frase, W., Wesler, M., Intrartikuläre Behandlung der Gonarthrose mit Zeel comp. – Ergebnisse einer Anwendungsbeobachtung Biologische Medizin 1996; 3: 115-119
Ricken, K.–H., Antihomotoxische Therapie als alternative vor cortison Wissenschaftlich symposium Brussel 16 november 1996
Thiel W, Borho B, Die Therapie von frischen Hämatrosen mit Traumeel Injektionslösung Biologische Medizin 1991 nr.2, 506-515
According to the teachings of Reckeweg’s homotoxicology, virtually every illness may be defined as either a defensive reaction by the organism against toxins or as the expression of toxic damage. It follows, therefore, that the blood of each patient contains those pathogenic poisons (homotoxins) typical of the disease from which that patient suffers.
Through withdrawing a patient’s blood, then homeopathically potentising it over several levels and subsequently re-introducing it by means of hypodermic injection, Reckeweg holds that precisely these pathogenic poisons undergo modification to yield a homeopathically active therapeutic agent ideal for application in stimulation therapy. This agent stimulates the body’s defense systems thus increasing detoxification and promoting the healing process.
According to Burgi’s Principle, the injection of appropriate homeopathic preparations intensifies efficacy of the potentised auto-sanguis blood to an even higher degree.
Auto-sanguis therapy is a treatment designed to exert a counteractive effect against exogenic and endogenic homotoxins (including toxic deterioration of by-products from the body’s own cells), thus promoting the healing of chronic disease in harmony with the laws of nature.
AUTO-SANGUIS: PROCEDURE
Withdraw 2–3 cc of the patient’s blood
Expell contents of syringe
Using the syringe and needle initially used for blood withdrawal, aspirate the appropriate Heel remedy (injeel, suis organ, etc.). It is best to use no more than 3 remedies. Once the remedy is in the syringe, cap the syringe and shake vigorously, about 10 times to potentise the mixture.
This is the first potentisation which is then injected into the patient s.c. or i.m. (and i.a. & i.p. in an experimental nature).
Intravenous injection is contraindicated in auto-sanguis therapy, as the degree of potentisation would be lost, and the intended action on the immune system would become questionable.
Potentisation can be carried out up to 5 times. The number of stages you select should be adjusted according to your prognosis, professional judgment and familiarity with the patient.
CONDITIONS THAT MAY BENEFIT FROM AUTO-SANGUIS THERAPY:
Iatrogenic conditions
Chronic viral and bacterial infections
Precancerous stages
Hepatic damage
Migraine
Chronic eczema
Bronchial asthma
Duodenal and gastric ulcers
Arthrosis
Lymphatic diathesis
PROTOCOL FROM A CASE STUDY Case study by: Drs Ivo Bianchi & Jo Serrentino
RE: 40 year old female Caucasian
CONDITION: Lower back pain due to strain and possible cervical hernia. X-rays showed a small deviation (less than 5 degrees) of vertebra #5, without arthrosis or calcification. This deviation was congenital and no damage seemed evident. The condition worsened because of irritation of the sciatic nerve due to overexertion.
PROCEDURE: 1–2 cc of patient’s blood was drawn into a sterile syringe. The blood was discarded, leaving only minute traces of the patient’s blood in the syringe. 2 cc of Discus compositum, 2 cc of Traumeel and 2 cc of Zeel were then aspirated into the emptied syringe (that still had traces of the patient’s blood). The injection was given s.c. in the region of the 5th vertebra.
RESULTS: Although this patient’s condition was not serious or degenerative, but rather from injury, it was very painful and restricted movement. A treatment to relieve and, mostly halt the progress of the condition, was imperative. The auto-sanguis treatment was followed with intravenous injection of Traumeel and with the oral administration of Zeel, Traumeel and Discus comp. fragmented over two weeks.
The patient claimed relief almost immediately, with a slight exacerbation within hours of the treatment lasting about 4 hours. The following day the patient was able to resume normal movement which progressively improved to full recovery without recurrence within the three year follow up period.
Neural therapy involves curative procedures which act via the autonomic nervous system. Techniques of neural therapy were developed from procedures applied for local anesthesis by the two brothers and general practitioners Dr. Ferdinand Huneke and Dr. Walter Huneke, both medical doctors in Düsseldorf.
Neural (Greek)
Of, relating to, or affecting a nerve or the nervous system.
Neuron
Nerve cell, nerve tracts, neuron theory
Neuron theory
The original version of the neuron theory, as published by Ramon y Cajal in 1934, stated that each nerve cell (i.e., neuron) represents an anatomical, genetic, functional, and regenerative unit.
The latest insights gained from electron-microscopic findings have confirmed the reality of synapses as physically and anatomically verified sites of junction: between two neurons (i.e., an interneuronal synapse) and between a neuron (peripheroreceptor) and the locus of action (i.e., a neuro-receptor synapse). These insights, in conjunction with complementary findings, represent the confirmed scientific basis for the entire fields of neurohistology, neurophysiology, and neuropathology.
The significance of neural therapy: Neural therapy involves curative techniques administered via the autonomic nervous system. The autonomic nervous system is a functional unit which includes the neurohumoral regulatory system in its overall mode of reflectoral operation. The autonomic nervous system encompasses the sympathetic nervous system, the parasympathetic nervous system, and the basic autonomic neural system. This basic autonomic neural system is the interstitial, soft connecting tissue which fills all organ interstices. It is composed of cells, nerves, capillaries, and extracellular fluid. This system plays the role of a communicator in the overall arrangement which enables each cell in the body to be in connection with every other cell. The autonomic nervous system is that part of the entire central nervous system which is of significance for the maintenance and reproduction of the particular organism involved. The autonomic nervous system primarily serves for control of the inner milieu. Since the control loops of the autonomic and somatic nervous systems are multiply interlinked at all synapse stages of the central nervous system, the functioning of the autonomic nervous system is not in fact strictly autonomous in nature.
The autonomic nervous system differs from the somatic nervous system in the following significant aspect:
Connections to the periphery are not uniformly present.
These connections are also subject to interruption by intermediate ganglionic stations (in which the ganglia are groups of nerve cell bodies). In the autonomic nervous system, sympathetic and parasympathetic ganglia are involved.
Human life is possible only in conjunction with the hermetic control of all regulation mechanisms. The pathways of the autonomic nervous system have the function of passing stimuli. Excessive stimuli disturb or block the development of energy and, in turn, the distribution of this energy. All neural therapeutic methods feature the introduction of energy to the impaired tissue, or they effect removal of the blockage by energy transfer. These procedures, however, also initiate reactions which are capable of eliminating damage which has already occurred. The body’s defense system, with its mechanisms of self-healing, is thereby stimulated to action.
All neural therapeutic techniques in the broad sense utilize this approach: acupuncture, chirotherapy, cutaneous and other types of stimulation, and cupping. And the same applies for neural therapy in the narrow sense: concerted injection therapy with local anesthetic.
HISTORICAL SUMMARY OF NEURAL THERAPY
Neural therapy by means of local anesthetic was discovered orientationally by Ferdinand and Walter Huneke. The Huneke brothers, both medical doctors from a family of physicians, had attempted unsuccessfully for years to treat their sister’s migraine attacks.
Atrophanyl, a new medication for rheumatism, was introduced onto the market in 1925. On the advice of a colleague, Ferdinand Huneke treated his sister by intravenous injection of the new preparation. The therapy immediately interrupted the migraine attack, with all its accompanying symptoms. Only one single subsequent administration, with the same success, was required to completely free his sister of her long-term suffering.
The two brothers were naturally impressed by the success of their treatment, but they could not explain the effects. They eventually determined, however, that Atrophanyl was available in the following two types:
For intravenous administration, without 2% addition of cocaine
For intramuscular administration, with 2% addition of cocaine
In his treatment of his sister, Ferdinand had confused the two solutions and had mistakenly administered the procaine solution intravenously – a form of administration which had until that time been expressly forbidden. It was believed then that procaine could damage important centers in the brain.
Motivated by the unexplained success of the therapy, the brothers then began to separately study the causative factors behind the accidental cure.
The two brothers independently discovered that the positive effect of the procaine was not only associated with the mode of administration (i.e., intravenous injection), but that the determining criterion for the therapeutic results was most probably the specific point of the injection. They wondered whether previously unknown reflex-type reactions could possibly act via Head’s zones.
Beginning with these findings, Ferdinand and Walter Huneke used injections administered at particular points to treat conditions of pain in the respectively segment-associated areas of the body. They named their technique “therapeutic anesthesia,” until Kibler, a friend, proposed a better name: “segment therapy with local anesthesia.”
In 1928, the Huneke brothers published their findings in Medizinische Welt under the title, “Unexpected Remote Therapeutic Effects of Local Anesthesia.”
Neural therapy as developed by the Hunekes is administered in two forms:
A. Segment therapy: Concerted injections of anesthetic into the segmental area associated with the illness.
B. Elimination of a focal disorder: Rendering a causal focal disorder ineffective by means of a neural therapeutic agent acts as causal therapy, with the elimination of complaints and pain in seconds (the so-called Huneke phenomenon), including pain without segmental association.
Definition of focal disorder
A focal disorder is chronically altered tissue which causes remote disorders via neural paths. A focal disorder is considered to be any pathological alteration which possesses the ability to cause remote disorders beyond its immediate locale.
Location of focal disorders
Pinpointing of the focus responsible for a disorder begins with preparation of a concerted case history, and includes systematic injections at potential foci.
SEGMENT THERAPY
Segment therapy is based on the insight that all parts of a bodily segment respond by reflection, as a unit, to particular processes. Stimulation pulses proceed from the body’s periphery, via the spinal cord, to the segment-associated organ, and vice versa. Pulses also travel along the dermato-visceral reflex path, or from an organ via the spinal cord to other organs—as well as along the viscero-visceral reflex path.
IMPORTANT: In all cases it is the entire human being which becomes ill, and never only one isolated organ. Concerted neural therapy not only interrupts pathological reflex paths, but also normalizes all autonomic neural functions through repolarization of the stimulus-disordered cell-membrane potentials.
Most important therefore is the point at which the injection is performed, and only to a lesser degree the particular medication which is administered. Segment therapy is genuine treatment in the original sense of the Latin origin “tractare,” to handle—a laying on of the hand.
Head’s zones
These zones were named for the work of Sir Henry Head, a London neurologist (1861–1940). These are hyperesthetic-hyperalgesic zones which appear on the surface of the human trunk in conjunction with disorders of certain inner organs, and which are characterized by heightened cutaneous sensitivity. This phenomenon has been explained by the fact that these cutaneous zones are provided with their sensitive innervation (nerve supply) from the same neural segments which supply the disordered organ.
Disordered sensitivity is also often found together with alterations of muscle tone (defense musculaire—for example, appendicitis), involving the viscero-cutaneous reflex.
What is meant by “chronically altered tissue”? Non-vital teeth, points of focal infection, tonsils as foci, scars on the surface of the skin or deeper in the body, scars on bones, foreign bodies, chronically inflamed organs (e.g., appendicitis chronica), and residual conditions after inflammatory processes which have subsided; e.g., in the ears and sinus cavities, at the gall bladder, at the appendix, in the female genital tract, and in the prostate.
HUNEKE’S INSTANTANEOUS PHENOMENON
In 1941, Ferdinand Huneke discovered that there are foci located on neural paths and not subject to any segmental assignment, yet capable of initiating and maintaining certain illnesses. These foci can be rendered ineffective in the neural-therapeutic sense by the concerted administration of local anesthetics. The disorders caused by the treated foci will then immediately vanish as a result of Huneke’s so-called flash phenomenon.
Huneke’s flash phenomenon is involved if all three of the following conditions are met:
All symptoms vanish instantaneously and completely.
Freedom from the symptoms continues for at least twenty hours.
The above phenomena are repeated with recurring symptoms.
If all conditions are met, injections are continued at intervals of one week—with the periods between injections gradually lengthened—until a complete cure is achieved.
Important: If, however, significant improvement is not achieved by injections into the segment, and if the flash phenomenon is not observed in the suspected focus, then injections at this point are futile, and the search for the proper focus must continue.
N.B.: The most important factor in neural therapy is the point of injection, and not the particular medication injected.
THE TECHNIQUES OF NEURAL THERAPY
Instruments required
Single-use cannulae
Single-use syringes (5‑ml plastic syringes have proved most effective for focal disorders)
A neural therapeutic agent.
Dosage and manner of application will vary considerably from case to case.
Wheal test
Raised, beetlike efflorescence with a red areola, as the expression of an acute edema of the skin.
Wheal test method: If a wheal applied intracutaneously with 0.2 ml of isotonic saline solution is no longer evident after 40 to 45 minutes, the patient has a propensity to develop edema. Disappearance of the wheals within 3 to 30 minutes indicates pronounced edema tendency.
DEFINITIONS
Neural therapy: Treatment of a disease via the autonomic nervous system.
Autonomic nervous system: A functional unity which includes the entire conditional-reflectorally functioning neuro-humoral system of regulation.
The autonomic nervous system includes:
The sympathetic nervous system
The parasympathetic nervous system
Basic autonomic neural system: An interstitial (i.e., located in intermediate tissue), soft connecting tissue which fills the interstices between organs. It is composed of cells, nerves, capillaries, and the extracellular liquid space. This system performs communicative functions required to provide connection between each cell of the body and every other cell.
Segment therapy: Therapy administered in a segment via Head’s zones. Deeper-lying organs are accessed via dermato-visceral reflex paths (as defined by Pischinger).
Focal therapy: If no success is achieved after repeated local or segment therapy, it may be assumed that a focal disorder is responsible for the complaint. It is then necessary to search for the responsible focus.
Local therapy: Direct administration of neural therapeutic agents which enables long-term freedom or relief from symptoms.
Procaine:p-aminobenzoyl diethylaminoethanol hydrochloride; the most frequently used local anesthetic; weak in its effects, non-toxic, and not harmful to human tissues.
Local anesthetic: An agent which, when locally administered, reversibly eliminates the excitability and conductivity of nerves or their endings. The area involved then becomes insensitive to pain.
Local anesthesia: Insensitiveness to pain in a locally restricted area of the body.
The efficacy of Lymphomyosot for the treatment and prevention of lymphatic disorders has been demonstrated in numerous studies¹–⁵.
Extremely well tolerated
In a study of 3,512 patients, including 1,124 (32%) children under 10 years of age, 99.8% assessed Lymphomyosot therapy as “very well tolerated” throughout the course of treatment¹.
3 different dosage forms
Drops: 15 drops 3 times per day
Tablets: 3 tablets 3 times per day
Ampoules: 1 ampoule 1 to 3 times per week
As a standard for comparison, 10 infusions with 600 mg of α-lipoic acid over 8 months improved tactile sensitivity among study patients by only Ø +0.9. However, a combination therapy with Lymphomyosot (15 drops twice daily for 8 months) and α-lipoic acid (10 infusions with 600 mg of α-lipoic acid over 8 months) improved tactile sensitivity by Ø +3.25⁵.
Neural nutrient insufficiency
Diminished tactile sensitivity
Defence reaction absent
Risk, imbalance, damage
Amputation
Gangrene
Diabetes
Diabetic foot
Inflammation
Malfunction/glycosylation of the matrix
Peri-neural oedema
Reduction of oedema
Severity of symptoms
Start
Reduction
No reduction
Slight
14
10
4
Moderate
26
19
7
Severe
0
9
1
50 patients diagnosed with diabetic neuropathy were administered 15 drops of Lymphomyosot twice daily for 8 months. At the end of the treatment period, lymphoedema and tactile sensitivity had profoundly improved⁵.
Improvement of tactile sensitivity
Severity of symptoms
Start
End
Difference
Slight
5.0
7.5
+2.5
Moderate
3.0
6.0
+3.0
Severe
0.0
3.0
+3.0
Minimizes the risks associated with diabetic neuropathy
Improved matrix metabolism
Improved tactile sensitivity
Eliminated pain in 75% of patients
Lymphatic disorders
Recurrent infections
Detoxification and drainage
Lymphomyosot – recommended for
Lymphhoedema (i.e. for promoting postmammectomy drainage)
A compromised defence system (i.e. for treating recurrent and acute infections, and inflammatory disorders such as tonsillitis or lymphangitis)
Tonsillar hypertrophy
Lymphadenitis
Systemic toxicities (i.e. for treating chronic diseases or amalgam-related disorders)
Indications: Status lymphaticus (tendency to hyperdevelopment of the lymphatic organs; tendency to development of oedemas and infections); glandular swelling; tonsillar hypertrophy; chronic tonsillitis. Contraindications: In case of thyroid disorders, this preparation may not be administered without prior approval from a physician. Side effects: None known. Interactions with other medication: None known. Dosage: Drops: In general, 15-20 drops 3 times daily. Tablets: In general, 3 tablets to be dissolved in the mouth 3 times daily. Injection solution: In acute disorders daily, otherwise 3-1 times weekly 1 ampoule i.m., s.c., i.d. Package sizes: Drops: Drop bottles containing 30 and 100 ml. Tablets: Packs containing 50 and 250 tablets. Injection solution: Packs containing 10, 50 and 100 ampoules of 1.1 ml. Revised: April 2001.
References
Zenner S, Metelmann H: Therapeutic Use of Lymphomyosot® – Results of a Multicentre Use Observation Study on 3,512 Patients. Biological Therapy 1990, Vol Vlll No. 3.: 49–53,67–72, and Vol Vlll, No. 4: 79–84, 94
Küstermann K, Weiser M: Treatment of a Lymphatic Disease with Homoeopathic Therapy. Biologische Medizin 1997; Vol 26 No. 3: 110–114
Rinneberg A-L: Lymphomyosot®: The Therapy of Tonsillitis and Prophylaxis against its Recurrence. Biological Therapy 1991; Vol IX No. 1: 111–114
Riley D, White S: A Biotherapeutic Approach to the Treatment of Inflammatory Disorders: A Drug Monitoring Trial. Biological Therapy 1992; Vol. X No. 3: 267–271
Dietz R: Possibilities of Lymph Therapy with Diabetic Polyneuropathy. Biologische Medizin 2000; Vol 29 No. 1: 4–9
Disorders of the ear, nose, and throat (ENT) are the cause of many patient visits to a primary care physician. Some of the common ENT disorders include acute and recurrent otitis media (OM); acute, chronic, and recurrent tonsillitis; and allergic and recurrent rhinitis and chronic rhinosinusitis (CRS). However, the common cold remains one of the most frequent upper respiratory tract infections (URIs). Approximately half of the cases of colds in children can be attributed to a wide variety of up to 200 different viruses that are seasonally active, such as rhinoviruses in the early fall, spring, and summer. Other viruses that might cause URIs include coronavirus, parainfluenza virus, adenovirus, enterovirus, and respiratory syncytial virus.¹
The subsequent development of recurrent sinusitis²–³ and OM⁴ commonly has been related to viral URIs that last longer than a week. A child can be expected to have 6 to 10 colds annually, whereas adolescents may have only 2 to 4 colds per year. In developing countries, URIs tend to be more severe, such as pneumonia and influenza, with a higher risk of complications. Therefore, URIs can be a leading cause of death for children younger than 5 years.⁵
An increased understanding of the pharmacoeconomic incidence, relevance of antibiotic resistance, physician involvement, and anatomical and physiological features of each of the common ENT disorders will improve clinical outcomes. An integrative medical approach that uses complementary and alternative therapies, such as antihomotoxic medications, in addition to mainstream medical therapies is a therapeutic strategy that shows much promise in reducing the current disease burden and preventing further recurrences.
Pharmacoeconomic Incidence
The annual cost of time lost from school for adolescents and from work for adults because of URIs is substantial and is estimated to be as high as $15 billion in direct treatment costs by practitioners, with more than half of that amount being for ambulatory care centers in hospitals. The indirect cost of wages from URIs is estimated at $9 billion.⁶
The over‑the‑counter cough and cold remedy market was identified as being the “most competitive category in North America,” with sinusitis showing the most potential growth. Figures extrapolated from a survey of 4,000 US residents suggested that a total economic burden of $40 billion, including income lost from time off for these occurrences, was related to noninfluenza viral URIs alone.
Antibiotic Resistance
In 2007, prudent antibiotic use was not correlated with appropriate knowledge of microbial resistance;⁷ thus, the reduction of unnecessary antibiotics as treatment options for the virally associated common cold was identified in 2008 as a public health priority.⁸
Recent public opinion polls show an increased understanding of the relationship between the development of resistant bacterial strains and inappropriate antibiotic use and also report a significantly higher level of trust in physicians who did not prescribe antibiotics for the common cold.⁹ However, 45% of respondents in the United States in 2008 and 41% of a population in Belgium in 2001 still did not understand the lack of efficacy of antibiotics in treating viral illnesses.¹⁰ These data suggest that there is still a considerable opportunity to better educate patients and health care providers.
Environmental Impact
In the pediatric population, the close proximity of children in day‑care centers contributes to the transmission of respiratory tract disease.¹¹ Childhood exposure to common environmental pollutants, such as firsthand or secondhand smoke, and common household allergens, such as aerosolized cleaning products, in persons with a genetic predisposition might be associated with later development of asthma and allergic conditions through inappropriate sensitization.¹² Furthermore, asthmatic children have URIs more frequently than their nonasthmatic classmates. The polycyclic aromatic hydrocarbons present in diesel exhaust particles have recently been shown to stimulate the release of interleukin (IL)‑4, IL‑8, and histamine from basophil cells,¹³ suggesting that other common environmental pollutants also can play a role in the development of asthma and allergic rhinitis.
Physician Involvement
Most persons with ENT disorders visit their health care practitioners early in the disease process because the associated signs and symptoms are readily apparent to both the patient and practitioner and frequently affect activities of daily living. The mechanical and physical appearances of structures (e.g., teeth, palate, gingiva, and tongue) indicate a variety of physiological states and can be used diagnostically with a minimal investment of time. For example, fasciculations of the tongue might indicate neural disorders; a glossy tongue is associated with nutritional deficiencies, such as a deficiency in vitamin B12. Dental caries or loss correlates with impaired immune systems, smoking or tobacco use or exposure,¹⁴ and poor nutritional status. Xerostomias are linked to poor hygiene, and temporomandibular joint disorders can be attributed to trauma or articular disorders.¹⁵
Relevant Anatomical and Physiological Features
Lymphatic tissue in the Waldeyer ring is designed to protect the body from pathogens and toxins encountered in this vulnerable area; therefore, it is strategically placed to protect critical respiratory and digestive functions. It is the first protective barrier encountered by orally ingested and inhaled toxins, viruses, and bacteria. An interaction with the body’s lymphatic tissues provokes a reaction that includes copious nasal discharge, sneezing, coughing, and mucosal engorgement as a mechanism to remove the offending substance. The resultant reaction, with its associated signs and symptoms, is diagnosed as the common cold or rhinitis. Further progression to include fever and exhaustion, and the presence of clusters of similar infections in the community and a documented influenza virus infection, would lead to a diagnosis of the flu.
Treatment for these uncomfortable reactions is largely symptomatic.
Pathological Conditions
A short review of the relevant pathological features of each of the common ENT disorders is included to provide further insight into potential therapeutic strategies.
Otitis Media
Acute OM Acute OM is the most frequent ailment encountered by pediatricians. Persistent middle ear effusion from a failure of the mucus and microbial and immune system debris in the middle ear to drain via the Eustachian tube to the pharynx is associated with recurrent OM.¹⁶ Implicated factors include functional obstruction of the Eustachian tube, anatomical differences in the infant’s Eustachian tube, and a more horizontal position when bottle feeding an infant in a supine position, favoring a retrograde flow of milk. Furthermore, passive smoke environments impair normal ciliary movement that sweeps away debris, and immune system disorders are associated with increased mucus production.
Recurrent OM Preexisting antibiotic treatment is associated with an increased rate of recurrent OM in young children, supporting the hygiene hypothesis, in which interruption of a normal inflammatory response during childhood leads to an imbalance in Th1/Th2 cell regulation, predisposing a child toward allergy.¹⁷ Novel otopathogens can be cultured in those with recurrent OM after a month‑long course of antibiotics for acute OM.¹⁸ Long‑term morbidity, with recurrent OM occurring before the age of 3 years, might affect the child’s subsequent decreased comprehension when reading.¹⁹
Bioregulatory Treatment For acute OM, use the basic/symptomatic approach as follows: prescribe Belladonna-Homaccord (8–10 drops twice daily) and Traumeel(8–10 drops or 1 ampoule warmed and instilled into the affected ear twice daily). If resolution does not occur within a reasonable time, individualize therapy:
With confirmed bacterial etiology and significant inflammation, prescribe Echinacea compositum: 1 tablet every 30–60 minutes up to 12 tablets per day for acute conditions; for chronic conditions, 1 tablet dissolved in the mouth three times daily. Injectable route (IM, SC, ID, or IV) 1–3 times per week may be used if within regulatory framework.†
With confirmed viral etiology, prescribe Engystol: 1 tablet three times daily or 1 ampoule daily (injectable routes as above for acute situations).
For marked restlessness, fever, and agitation, prescribe Viburcol suppositories: adults, 1 suppository 2–3 times daily; infants under 6 months, half a suppository up to one per day.
If signs and symptoms persist, consider the 3‑pillar regulation approach (detoxification and drainage; immunomodulation; cell and organ support).† During latent phases, Mucosa compositum (± Coenzyme compositum, Ubichinon compositum) supports cells and organs; Traumeel for immunomodulation; and the Detox‑Kit (comprising Lymphomyosot, Nux vomica-Homaccord, and Berberis-Homaccord) for detoxification and drainage. Persistent effusion may require referral for myringotomy.
Tonsillitis
Acute Tonsillitis Tonsils are antigen‑presenting lymphatic tissue in the Waldeyer ring, mounting an appropriate B‑cell response. Acute tonsillitis presents as erythematous, swollen tonsils with stertorous breathing. Hypertrophied tonsils can cause sleep disorders and daytime inattentiveness in children. Microbiological evaluation (culture or rapid antigen tests) is required to exclude streptococcal pharyngitis, which necessitates antibiotics to prevent cardiovascular or renal complications.²⁰
Chronic Tonsillitis Generally bacterial in etiology and more prevalent in adults. Crypts containing pus can form; surgical excision is controversial due to postoperative pharyngitis despite no visible recurrent infection. Post‑tonsillectomy changes in oral flora suggest the chronically infected tonsil may harbor anaerobic bacteria, and removal may restore normal flora.²¹
Recurrent Tonsillitis In children, recurrent tonsillitis differs from adult chronic forms by higher antigen presence in acute stages. If peritonsillar abscess occurs, immediate tonsillectomy may be first‑line.²² Antigen presentation and B‑cell function remain intact; if possible, avoid tonsillectomy to preserve natural killer cell maturation.
Bioregulatory Treatment For acute tonsillitis: prescribe Angin-Heel (initial: 1 tablet every 15 minutes for 2 hours; then 1 tablet three times daily), Vinceelspray (once daily), and Mercurius-Heel (1 tablet three times daily). If unresponsive: