FEATURE ARTICLE
Practical Empiric Therapeutics with Biotherapeutica-Antihomotoxica in Geriatrics
DR. MED. H.-D. NOESKE
Summary
As present-day findings show, a biological therapy form should be preferred for the elderly.
The aim of a biological therapy for old people should be:
- to relieve the organism as far as possible of pathogenic loads and harmful noxae
- to support the regeneration possibility of the cell structures
- to activate the molecular-biological functions of the cells
With this multitude of processes, the therapy must be manifold:
- The diseases in senium are to be relieved by an antihomotoxic therapy with homeopathica, nosodes and biotherapeutica.
- The cells of the parenchymal organs, the vessels and the ubiquitous mesenchymal tissue are to be supported and activated with the help of organ preparations.
- The intermediary metabolism functions of the cells are to be improved through the catalysts of the citric acid cycle, through minerals and vitamins.
A healthy way of living is part of the therapy:
- The old person should remain active.
- Fresh air is necessary.
- Hygiene and body care must be stressed.
- The surroundings of the old person should be psychologically well-balanced.
- The diet should be mainly lactovegetarian. The maintenance of the right amounts of protein, carbohydrates, fats, vitamins and minerals is the basis of a healthy diet.
The following basic therapy has proved to be effective:
- The oral medication with Galium-Heel, Psorinoheel, Crataegus, Cralonin, Cocculus compositum and Secale compositum.
- Symbiosis control, as advised by Mommsen and Kolb.
- The vitamins A, E and C should be prescribed repeatedly.
- The prescription of minerals. Especially calcium, iron, magnesium, copper and potassium are needed in old age.
- A constitutional medicine prepared according to the classic rules of homeopathy should be prescribed now and again.
The therapy suggested here is for the aging but still healthy person who seeks advice and help in the surgery. If older persons suffering from geriatric diseases come to the surgery, then a therapy plan can be widened according to the diagnosed health disturbances and an additional causal treatment can be carried out.
To make the problem more understandable, I would like to widen the theme and consider aging, the complaints and their treatment. It is not intended here to give just a catalogue of treatment instructions. On the contrary, the attempt will be made to present guidelines for a biological treatment of aging persons. Naturally, therapeutical information and advice will be stated. However there is no claim to completeness as in a textbook. What is given are solely practical experiences.
I would like to ask you to join me in reflections and thoughts regarding biological aging and health disturbances in this life phase. The necessary treatment can only be derived from the knowledge of the aetiology of these psychological and pathological processes.
The statements are divided into:
- Preliminary remarks regarding the problem of aging and geriatric diseases
- Therapy:
a. General Guidelines
b. Basic Therapy
c. Practical examples
- Remarks regarding retardation and alleviation of biological aging
1. Preliminary remarks regarding the problem of aging and geriatric diseases
Having reported several years ago regarding homotoxicological problems in geriatrics and having already tried to make treatment suggestions, certain research results and facts should now only be called back to mind very briefly.
At that time, various theories regarding aging were reported on. According to Hayflick, the symptoms of old age are caused by a loss or so-called mistakes in the genetic information of the cells, according to Hahn by a function loss of the intracellular regulation processes and according to Robert by synthesis disturbances of the connective tissue, whereas Burnet sees aging as an increasing weakening of the immunological control of the organism.
Summarizing these reflections, it can be stated, according to the research results, that the aging processes take place on the molecular and genetic level of the cells and result in morphological and biochemical changes of the organs (Platt). These physiological changes during aging are often superimposed by pathological aging mechanisms. A further observation is in fact that with increasing age, the number of diseases increases, that could also occur during a younger age. There is thus the possibility that several diseases appear at the same time—this is the so-called “multimorbidity”. The most conspicuous factor is however, that there are no specific diseases of old age, but rather a sum of health disturbances during this phase of life.
In some cases it is not possible to distinguish between the age processes with their complaints and the diseases. The borders are blurred, the transition is flowing. Our patients are people with health disturbances that occur in this phase of life, when the catabolic outweigh the anabolic metabolism functions of the organism.
Some more explanations and information should be given regarding this.
Findings in morphology show that aging processes can be observed in all life phases. Young and old mesenchyma and parenchyma cells co-exist continuously. It is known that in nearly all organs the collagen content increases with increasing age, the number of fibroblasts is reduced and the turnover rate of the parenchyma tissue decreases (Lindner). The regenerative power of the cells deteriorates. Tests regarding old age show that changes due to old age are caused by an activity reduction of certain key enzymes of the collagen metabolism (Lindner).
A further morphological finding is that amyloid deposits are a sign of accelerated aging processes. Pathology however shows us that increased amounts of amyloid can be observed in the case of chronic inflammation. This process could lead our thoughts to the homotoxins (Reckeweg), as homotoxins are all those toxins that are caused by diseases and that deposit in the tissue.
The molecular and genetic function changes and disturbances of the old person take place in the mesenchyma, in the DNA of the nucleus and in the cytoplasm of the cells.
The findings by Pischinger and his collaborators regarding the mesenchymal basic system show that this ubiquitous active tissue is switched before the parenchymal organelles. All the physiological and pathological processes of the organism take place in it. It builds the transit route to the tissues, vessels and nerves. If the mesenchymal stroma is strained or diseased, the organ after it is also affected adversely. The mesenchymal basic system contains the homotoxins described by Reckeweg which affect the organelles from here with all pathogenic possibilities.
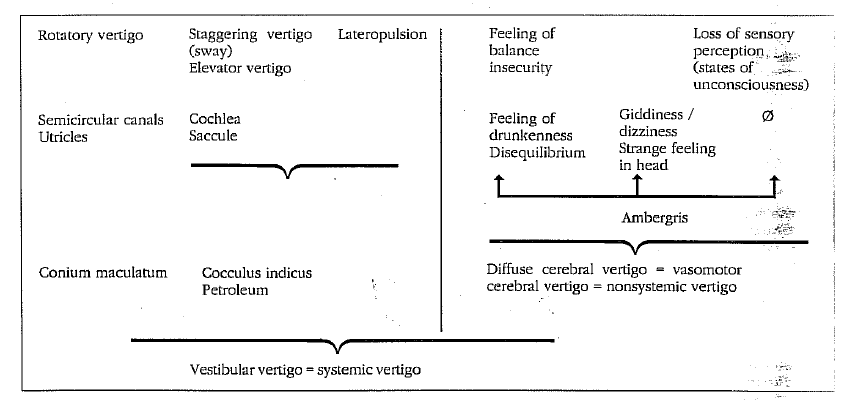
For this reason Voll has been teaching for more than two decades that to maintain the health of an organism and as a prerequisite for recovery, the mesenchyma must be reactivated – or as we used to express it – cleaned out. Moreover, morphological and biochemical tests showed that with increasing age, intramural, arteriosclerotic metaplastic processes can be observed in the vessels of the parenchymal organs. These changes typical for old age are followed by a reduction of the number of cells – i.e. atrophy – and by functional disturbances of the organs supplied by these vessels. This leads, therefore, for example, to a reduced output capacity of the cardiac musculature with the corresponding consequences, or it can lead to clouding of consciousness and disorders of balance in the brain and labyrinthine system as well as to a change of the concentration power and clearance of the kidneys.
All these changes of the organs typical for old age should also be taken into consideration when determining a therapy for the aging or old person, as, considering what was just said, chronic and multiple pathological effects can be expected. Medicine, e.g. antibiotics, that is mainly eliminated renally, can accumulate more easily and lead more quickly to side effects than would be the case with younger people. In old age the limit of tolerance for glycoside at the previously damaged heart is also changed.
With these findings and the knowledge of the outlined, many research results, a biological therapy form for senium should be preferred, as far as it is practicable, even if only to decrease or eliminate the possibility of the side effects of medicine.
The aim of a biological therapy for old people is therefore:
- to relieve the organism as far as possible of pathogenic loads and harmful noxae,
- to support the regeneration possibility of the cell structures and
- to activate the molecular-biological functions of the cells.
As the attending doctor must reckon with a multifactor aging process and with a geriatric patient with multimorbidity, the treatment must be multilayered, if not to say it should correspond to a direct polypragmasy. Above all, it should not be directed only at the symptoms complained about, but should also take into consideration the patho-physiological processes that led to the complaints in this phase of life.
The treatment approach therefore should be many-sided:
- With an antihomotoxic therapy using homoeopathica, nosodes and biotherapeutica, not only the aging process should be delayed but also diseases in senium should be improved.
- The cells of the parenchymal organs, the vessels and the ubiquitous mesenchymal tissue are to be supported and activated with the help of organ preparations.
- The intermediary metabolism functions of the cells are to be improved through the catalysts of the citric acid cycle, through minerals and vitamins.
It is also important for the therapist to know the personal anamnesis of the aging patient. I consider this to be of more importance than it already should be for younger persons who are ill, as there are fewer psychophysical compensation possibilities during the aging phase. Making a geriatric anamnesis requires patience, time and understanding.
In this connection I would like to mention that in my surgery I try to use the electro-acupuncture method according to Voll to make a diagnosis and make tests to determine each individual therapy. This method has often been of great help to me when making a diagnosis, considering the changed reactions of older persons and their often incomplete information about their complaints.
2. Therapy
a) General Guidelines
There are some general guidelines for a healthy way of living, before going on to the basic therapy:
1. The old person must remain active. Movement, walks and physical training help the older person to maintain flexibility and fitness and to prevent geriatric diseases.
2.Fresh air – if possible containing O₂ – is necessary.
3.Hygiene and body care should be stressed, as the old person is often no longer able to look after himself on his own.
4.The surroundings of the old person should be psychologically well-balanced. There should be understanding and respect for his age, his complaints and his own particular character.
- His diet should be mainly lactovegetarian. As the enzyme activities are reduced during old age, the reaction processes in the intermediary metabolism are also slower. The maintenance of the right amounts of protein, carbohydrates, fats, vitamins and minerals is the basis of a healthy diet (Halden). Nicotine is forbidden, only small amounts of alcohol are allowed.
For these reasons natural and unprocessed food is an effective protection against premature decrease in vitality and diseases. The lipotropic substances of milk products have a less adverse effect on the liver as a metabolic organ than a mainly meat diet. Besides, a lactovegetarian diet helps to normalize the fat and cholesterol metabolism. If the diet contains a lot of meat, there is an increased need for magnesium for the enzymatic protein digestion. Magnesium can be found in the chlorophyll of leafy vegetables and in whole meal products. As the normal diet nowadays contains only reduced amounts of these foods, the result may be a magnesium deficiency syndrome (Halden).
b) Basic Therapy
The following medication has proved to be successful:
- Oral medication, prescribed every few months as a cure:
Galium-Heel, Psorinoheel, Cocculus compositum, Crataegus, Cralonin and Secale compositum
- Symbiosis control, as advised by Prof. Mommsen and Dr. Kolb
- The vitamins A, E and C should be prescribed repeatedly.
- Vitamin A is the vitamin for the mucous membranes and the visual purple;
- Vitamin E is considered the vitamin for the metabolism of the connective tissue, it also stimulates the anterior pituitary lobe and inactivates the free radicals that bring about aging processes at the mitochondria, the energy center of the cells, according to Haman.
- According to Prof. L. Pauling, vitamin C increases the defensive powers.
- Minerals: They are prescribed after a diagnosis has been made using full blood. According to experience, the old person needs mainly calcium, iron, magnesium, copper and potassium.
- The homeopathic constitutional medicine must be determined according to the rules of classical homeopathy and should be prescribed for the old person from time to time. The individual reactive and defensive powers of the patient can be influenced favourably by prescribing high potencies.
The measures suggested so far are for the aging but still healthy person, who comes to our surgery seeking advice and help. If older people come to us for treatment suffering from so-called geriatric diseases, then the therapy plan is widened according to the diagnosed health disturbances and the stated reflections.
c) Practical Examples
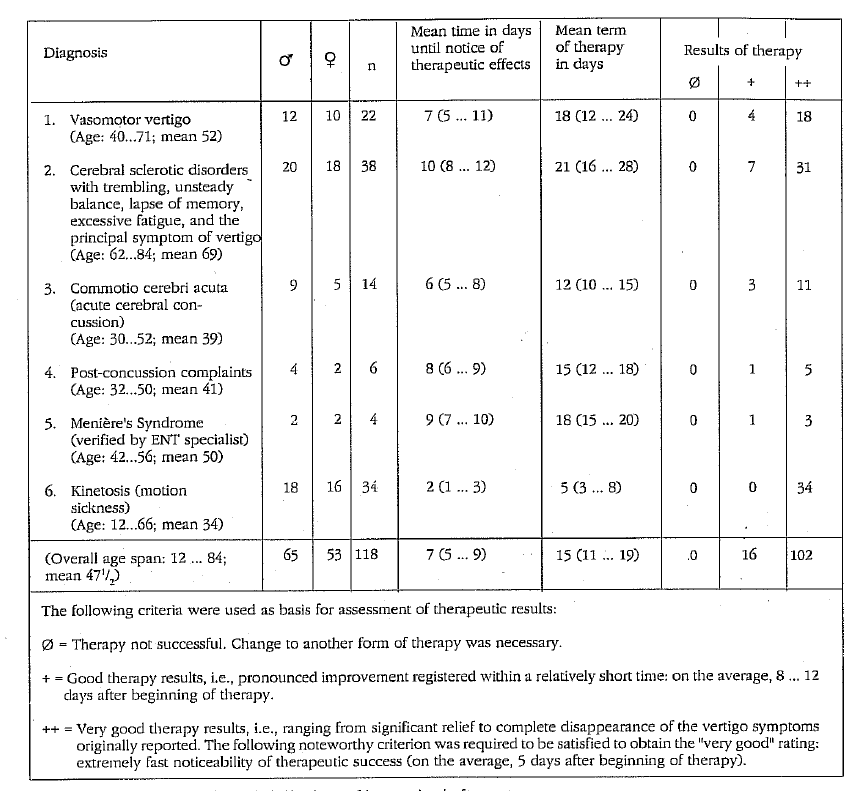
I cannot provide any statistics here regarding treatment results; only a few examples from fields of internal medicine that show the difficulties of geriatric diseases, the complaints and treatment possibilities. I must point out that I do not treat solely geriatric cases; my patients are people seeking biological treatment.
1st treatment example:
85-year-old man complains of “catarrh” of the respiratory tract, coughing up in the morning, watery nose secretion during sneezing, thick voice, extreme fatigue is obvious. Has had these complaints for several months; they are the rest of a so-called “cold”.
The examination showed:
Chronic sinusitis, chronic tonsillitis and a bronchitis with emphysema, brought about by influenza viruses and Coxsackie virus B4. The heart was strained by the virus infection and the chronic bronchitis, however there was no heart insufficiency. Furthermore the examination brought to light disturbed bacterial flora in the small and large intestines with an enzyme deficiency syndrome and chronic colitis as well as a cholangiopathy and a venous circulatory disorder of both legs. Asked directly after the examination, the patient mentioned suffering from meteorism, tendency to obstipation, bloating after meals and fat indigestion.
The therapy consisted of:
Injections of Echinacea compositum, Lymphomyosot, Galium-Heel, Natrium oxalaceticum-injeel, Silicea-injeel as well as Coxsackie-Virus-B4-Nosode-injeel, Influenzinum-Nosode-injeel, Sinusitis-Nosode-injeel, Tonsillitis-Nosode-injeel, Staphylococcus-injeel, Streptococcus-haemolyticus-injeel, Pneumococcinum (Klebsiella pneumonia-injeel) and Polypus nasalis-injeel. Also prescribed were the “organ preparations” Mucosa compositum, Cor compositum and Glandula thymi suis-injeel.
The oral medication consisted of the following:
Lymphomyosot, Cralonin, Husteel, Naso-Heel and Leptandra compositum.
The constitutional medicine was Natrium muriaticum. The patient’s condition improved with this medicine. The catarrh became less and as a result, likewise the sneeze and cough irritation. The homeopathic medicine Natrium muriaticum greatly improved the patient’s general health.
Therefore, some information about the “so-called digestion complaints” of older people. These complaints usually are caused by an enzyme insufficiency syndrome and a disturbed bacterial flora in the small and large intestines, often in combination with a pankreopathy and cholecystopathy or cholangiosis. There can be various symptoms; the complaints are described differently.
Each person experiences different disturbances. Most people complain of obstipation. But there are also many patients for whom a thin, pasty or rarely formed stool is normal. Further complaints are a sensation of fullness or pressure in the epigastrium after meals; they cannot “belch”. Some others suffer from heartburn after easily digestible carbohydrates, especially after eating cake.
In the case of the first treatment example, the patient reported suffering from indigestion, besides difficult breathings. The indigestion problem was only admitted upon direct questioning. As it turned out, he had been having these difficulties for years. They were now a part of him. He had integrated them into his life.
This seems to be typical for older people, that is, to accept their complaints as typical, to adjust themselves to them, often to thrust them aside and only when questioned directly to admit having them with the words: “Yes, of course, I’ve had that for ages”. Or is perhaps this psychological process of repression a purposeful mechanism of nature?
For patients with indigestion the following therapy has proved to be successful:
Oral: with meals an enzyme preparation, after meals Chelidonium-Homaccord or Hepeel; in addition, symbiosis control.
In the case of acute disorders, Gastricumeel and Duodenoheel are prescribed, in the case of diarrhoea the preparation Veratrum-Homaccord or Diarrheel, in the case of bloating, Carbo vegetabilis-Injeel.
As injections for acute disorders Erigtoheel, Injeel-Chol, Veratrum-Homaccord, Mucosa compositum and Engystol are prescribed. According to the diagnosed organic disorder, the corresponding nosodes and organ preparations should be injected in combination with catalysts.
2nd treatment example
A 75-year-old woman complains of disequilibrium when changing position, especially when getting up and straightening up after bending, also of pressure in her head and insomnia despite extreme fatigue. She had been having these complaints for several weeks, while treatments by others had not helped. During further recording of the case history, she complained of “cold fingers”. Sometimes – when she is in town – she goes into a café, to order a cup of coffee; not to drink it, but to warm her fingers in it.
The examination of this patient brought to light a considerable arteriosclerosis, a spondylosis and osteochondrosis of the cervical vertebral column as well as chronic polypous inflammations of the paranasal sinuses.
The following were prescribed as injections:
Vertigoheel, Cerebrum compositum, Traumeel, Circulo-Injeel, Mucosa compositum and Sodium oxalaceticum-injeel. In addition the organ preparations: Art. basilaris, Art. vertebralis, Circulus arteriosus cerebri and Proc. mastoideus.
Ferrum phosphoricum was prescribed as a constitutional medicine. For external reasons the injections were given elsewhere. Several months later the patient came to me again, complaining of backache. Asked regarding the disturbed circulation and this disequilibrium, she said that her condition had got better after a few injections and she had not had the complaints again.
With increasing age older persons suffer increasingly from a latent cardiac insufficiency, especially combined with the symptoms of a load insufficiency, a general decrease of vitality and disturbance of sleep. A latent cardiac insufficiency can turn into a manifest cardiac insufficiency, especially when there are additional loads, e.g. infections. Causal are, among other things, the already mentioned arteriosclerosis of the small intramural coronary arteries, the cardiovascular senile amyloidosis and the multimorbidity that is also valid for the organ heart. Moreover tests made by pathologists show that with increasing age, the functional capacity of the heart decreases yearly by an average of 1% of the capacity at the age of 30.
As a prophylactic treatment of the old heart, that shows no signs of insufficiency, the following preparations from Heel are used:
Cor compositum, Hepar compositum, Magnesium-manganese phosphoricum-Injeel and Carbo vegetabilis-Injeel as a mixed injection, and at the same time Cralonin orally.
In the case of a more extreme coronary arteriosclerosis, Placenta compositum and the corresponding organ preparations with their accompanying therapy are prescribed additionally. If there are rhythm disturbances then it is advisable to use Cactus compositum, Glonoin-Homaccord, Chelidonium-Homaccord and Cralonin. Should there be a heart insufficiency, glycosides should be prescribed, as the biotherapeutica mentioned would not be sufficient for such a severe clinical picture. The serum-potassium level must be controlled.
3. Remarks regarding retardation and alleviation of biological aging
The retardation of aging and the alleviation of a person’s last life phase is a prophylactic task with which we are confronted again and again in the surgery. Everyone would like to maintain his psychophysical capacities and health for as long as possible. It follows from the deliberations stated at the beginning that aging is a biological process. On the other hand, it is known that pathological loads that reach the organism via its mesenchyma, whether of viral, bacterial, chemical or physical origin, lead to degeneration of the organs, vessels and nerves and thus to premature aging of the individual. For this reason preventative measures are important for older persons.
Prerequisite for a successful treatment are the guidelines for a healthy way of life and healthy diet mentioned at the beginning of this article. These are followed by the drug therapy that has the target of retarding the normal aging process.
After the EAV test, I regularly try in my surgery to reactivate the mesenchyma using nosodes and an accompanying homeopathic therapy.
The purpose of the therapy is also to strengthen the cells and their structures. This is possible with organ preparations. Also the molecular-biological functions that are connected to the cell structures can be supported by additional doses of potentiated catalysts of the citric acid cycle (Heel); intermediary metabolic factors and minerals. I use potentiated organ preparations for this.
The aging patient should be given mainly organ preparations for the immune system, as for example Thymus, Nodi lymphatici, Medulla ossium and Hepar. The ubiquitous mesenchymal basic system can be strengthened with the preparations Mesenchym and Funiculus umbilicalis. In the same way the other organs can be treated with the corresponding suitable organ preparations. The medication mentioned in the basic therapy should be prescribed additionally from time to time.
With these statements I wished to point out the therapeutic possibilities given with a biological therapy for the aging process and geriatric diseases. With the help of biotherapeutica-antihomotoxica the old person can be spared disorders without any side effects. The diseases of old age can be influenced positively, to a great extent, by these medications.